Download
1 / 35
360 likes | 512 Views
Micro-Systems in Health Care: Essential Building Blocks for the Successful Delivery of Health Care in the 21 st Century. Thomas P Huber, MS ECS September 18 & 25, 2006. Presentation to CCHA/CCS NICU Improvement Project . Aim of Presentation.

E N D
Micro-Systems in Health Care: Essential Building Blocks for the Successful Delivery of Health Care in the 21st Century Thomas P Huber, MS ECS September 18 & 25, 2006 Presentation to CCHA/CCS NICU Improvement Project
Aim of Presentation Introduce the Clinical Microsystem Improvement Framework as a way of continually improving unit performance as well as enhance your understanding of quality improvement methods, theories, tools, and techniques.
AGENDA • A Brief Introduction • So . . . What’s a Microsystem? • Dartmouth - RWJ Study on Microsystems • The Clinical Microsystem Action Guide & the 5 P’s Framework • Improvement Tools, Advising Approach, and some key Learning's over the years!
So . . . What’s a Microsystem • Definition • A Picture View • Examples • Shrek’s “Onion Persective” of Microsystems • The Current Reality Problem
Definition A micro-system in health care delivery can be defined as asmall groupof people who work together on a regular basis to provide care to discrete subpopulations ofpatients. It has clinical and businessaims, linkedprocesses, sharedinformationenvironment and produces performanceoutcomes. They evolve over time and are (often)embeddedin larger organizations.
Microsystems are thebuilding blocksthat come together to form Macro-organizations Walk around in a health delivery system with microsystem glasses what might you find? • An Emergency Care Center • Asthma and Allergy Clinic • Day Surgery Center • A Nutrition Clinic • A Neonatal Intensive Care Unit
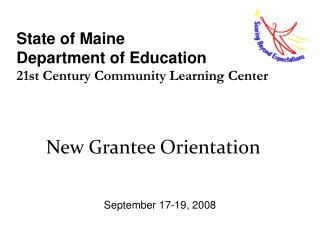
The “Onion” Perspective on Levels of Quality Improvement! Community, Market, Social Policy System Self-care System Macro-organization System Micro-system Individual care-giver & patient System
When we connect things that don’t match... The Economist
Dartmouth - RWJ Foundation Microsystem Study (2000 - 2003) Joint Commission Journal Article in your Packet. The search for 20 high performing microsystems How we studied and worked with the microsystems A few Examplesof Excellence The Results: The 10 Success Characteristics of high performing microsystems & the 5 P Framework
The Search for High Performance?Dartmouth-RWJ Study: Batalden, Nelson, Huber, Mohr, Wasson, Headrick. 2000 - 2003 • Identified 250 high performing healthcare microsystems via a multi-stratified approach. • Screen 75 microsystems using (MS Assessment Tool and 30-Min Telephone Semi-Structured Interview (Q, $, and Process). • Selected 20 microsystems across the healthcare spectrum: Ambulatory, Inpatient, Nursing Homes, and Home Health.
Ambulatory Care (Primary) MacroMedical MGH, Boston, MA Norumbega Medical, Bangor, ME ThedaCare Family Practice, Kimberly, WI Grace Hill CHC, St. Louis, MO Ambulatory Care (Specialty) Intermountain Ortho, Boise, ID Overlook Hospital Emergency Department, Summit, NJ Sharpe Diabetes Center, San Diego, CA Spine Center, DHMC, Lebanon, NH Washington Cancer Institute, Orthopedic Oncology, Washington, DC Inpatient Care and Same Day Surgery Henry Ford-NICU, Detroit, MI IHC Shock Trauma Unit, Salt Lake City, UT Shouldice Hospital, Hernia Repair, Toronto, Canada Mayo Luther-Midelfort, Behavioral Health, Eau Claire, WI Nursing Home and Hospice Care On Lok SeniorHealth, San Fran, CA Iowa Veterans Home, Marshaltown, IA Bon Secours Maria Manor Nursing Center, St.Petersburg, FL Hospice of Iowa, Mason City, IA Home Health Care Gentiva, Rehab without Walls, East Lansing, MI Visiting Nursing Service of NYC, New York, NY Interim Healthcare, Pittsburgh, PA The 20 Finalists
How good is good? a few results. • Mass General Hospital Primary Care • Waiting Room time – how many minutes? • Shouldice Hernia Hospital • OR turnaround – how many minutes? • Disposable costs per operation? 8 Minutes or the Co-Pay is waived 1 Minute and 30 Seconds versus 90 min $17. 50 versus national average $500
Study Results 10 Success Characteristics of High Performing Clinical Units Step 1: Review Handout and complete the Microsystem Assessment The 5 P’s: Purpose, Patients, Professionals, Processes, and Patterns Step 2: Review document and work on Professionals and Process Handout
We found 10 Success Characteristics that are associated with high performance Strong Leadership Great Organizational Support Focus on Staff (Professionals) Education and Training of Staff Interdependence of Care Team Performance Result Focused Process Improvement Focused Patient-Centered (Patient Focus) Community and Market Focus Information & Information Technology Orientation
Clinical Microsystem Assessment Exercise Instruction: each of the “ 10 success characteristics” (e.g., leadership) is crucial for high performance. Below each of the characteristics is defined and is followed by a ranking from 1 – 5 (low – high) as well as 3 descriptions (low – high performance). For each characteristic please circle a number 1 – 5 that best describes your current Microsystem. 1. Leadership: The role of leaders is to balance setting and reaching collective goals, and to empower individual autonomy and accountability, through building knowledge, respectful action, reviewing and reflecting. 1 2 3 4 5
The 5 P’s of Micro-systems include ... • Purpose - Our aim and mission. • Patients - Our reason for doing our work. • Professionals - Our staff who work in the trenches to take care of patients. • Processes - Our system of inter-related events that constitute the microsystem. • Patterns - Our way of doing our work (Measurements, Data, Run Charts)
Purpose Patients Processes Patterns Professionals
The 5 P’s of Micro-systems include ... Purpose The purpose is our aim and mission: What are we trying to accomplish? An explicit statement summarizing what is expected to be achieved from the improvement initiative. Helps to maintain focus on a specific opportunity or problem during the project. Helps to identify appropriate members of the improvement team. Pgs 103, 104 in Action Guide
The 5 P’s of Micro-systems include ... Patients Patients are the reason for doing our work. What is the target population age distribution? Ave. Length of Stay? Mortality Rate? List your top 10 Diagnosis Pt. Population Census Additional patient information, ______________? Family Surveys, Capturing patient information on an ongoing basis . . . PGS 59 – 70 in Action Guide
The 5 P’s of Micro-systems include ... People (Professionals) Professionals - Our staff who work in the trenches to take care of patients. Complete the Handout Pgs 11 – 15, including: Who is part of your team, list out staff and %FTE Complete Staff Satisfaction Survey Complete Inpatient Unit Personal Skills Assessment Complete Inpatient Unit Activity Survey Sheet
The 5 P’s of Micro-systems include ... Processes Processes - Our system of inter-related events that constitute the microsystem. Inpatient Unit Patient Cycle time, Handout Pgs. 16 Inpatient Unit Know Your Process - Core and Supporting Processes, Handout pg. 17 Flowchart core process related to nosocomial infections See Handout Pgs 16,17 & Action Guide Pgs. 116 – 122 (Detailed Overview of Flowcharting)
The 5 P’s of Micro-systems include ... Patterns Patterns - Our way of doing our work (Measurements, Data, Run Charts) Capture key clinical data related to nosocomial infections, and line infection rates What measurements are being captured? Definitions, Data Owner, Current and Target Values, Action Plan and Process Owner See Action Guide: Pgs 70 - 82
Healthcare Improvement Tools and Our Advising Approach Tools in the Clinical MS Action Guide MS Advising Approach Key Learnings from Microsystem Work A Concluding Remark
Microsystem Tools and Resources • A Clinical Microsystem Action Guide (www.clinicalmicrosystem.org) Tools and Resources - A Map for Improvement • (General) Clinical Microsystem Profiler, Pg 14 • (Professionals) Practice Staff Profiler, (see handout) • (Process) PDSA, Plan Do Study Act, Pg. 112 - 114 • (Patients) Patient Flowcharting, Pg. 15 • (Big Picture) Clinical Microsystem Picture, Pg. 22 • (Patterns) Performance Patterns: Measurement and Monitoring, Pgs 70 - 82 • (Process) Fishbone Diagrams, Pgs 115 - 116 • (Big Picture) Clinical Microsystem Assessment Tool, Pgs 16 - 19 • (Safety) External Environment, Health Professional Education Pgs 102, 103 • (Purpose) Aim Statement, Vision and Mission Journal, Pg 103, 104 • (Professionals) Meeting Agenda Graphic, Pgs. 103 - 109
Microsystem Advising Approach The Clinical Microsystem Action Guide along with years of accumulated knowledge in CQIprojects creates a ROADMAP for improving care at the Unit Level. Phase 1: Build MS Awareness via Assessment & Diagnostic Tools • Complete Microsystem Assessment Tool. • Pick Options in action guide, which Tools to use, set goals (What, Who, and How of project). Phase 2: Gather Data, Flowcharting & Mapping Processes • Do a site visit & interviews, and capture key Q, $, & Process Measures. • Patient & IT Flowcharting, Small work group meetings. • Foster “MS & Improvement Culture”.
Microsystem Advising Approach The Clinical Microsystem Action Guide along with years of accumulated knowledge in CQIprojects creates a ROADMAP for improving care at the Unit Level. Phase 3: Data Crunch, Analyze Q, $, & Process Measures • Crunch and analyze the data (project specific measures). • KEEP ENERGY HIGH for project, support support support! • Provide on-going feedback of measures (Patterns). Phase 4: Finish Work, Present Outcomes, Work on Spread • Congratulate and Celebrate Successes. • Review what we learned, provide feedback, and document changes. • Plan for next phase (Intra-Unit and Inter-Unit Spread), Utilize High Energy from project for spread.
IHI workshops, symposium, teaching, and training Microsystem assessments, and CQI work at various Clinics Culture Redesign: e.g., NICU Dartmouth Lahey Hospital Strong Vision and Mission is needed - at the unit level (Purpose). We need strong local and senior leadership for real change to happen. Do interviews, gather objective data, manage the process, be alert for hidden gems (LHF). Work at the microsystem level for effective lasting change . Include the right staff, facilitate conversation, be open to surprises. Emphasize fluidity and flexibility during the spread of change. Learning from Eight Years of Microsystem and CQI Work
Redesign, IT Infrastructure, Change Management: 27 Kaiser Intensive Care Units Patient and Information Flow (lean thinking): e.g., Keene Clinic Redesign Technology Adoption: UCSF - Stanford Hospitals The Planning Phase is crucial in PDSA, and critical for HER. First map the processes then implement the HER. Mapping processes creates energy, highlights areas for change, and gets staff buy-in. Having an outside support person is helpful in lean thinking mapping. Work with underlying (hidden) agendas to make changes. Use the creativity of the Professionals(they know what needs to be done). Learning from Eight Years of Microsystem and CQI Work
Concluding Remark Healthcare organizations might not be utilizing the term micro-system, but it is clear that many high quality and cost-efficient providers are organizing themselves around functional front-line teams & professionals that have the right information at the right time, to deliver the best care possible.
If you want to learn more . . . References • Thomas P. Huber, M.S.; Paul B. Batalden, M.D.; Eugene C. Nelson, D.Sc., M.P.H.; Marjorie M. Godfrey, M.S., R.N.: “ Microsystems in Health Care: Developing People and Improving Work Life: What Frontline Staff Told Us.” The Joint Commission Journal on Quality Improvement, October 2003, Volume 29 Number 10. • Eugene C. Nelson, D.Sc., M.P.H.; Paul B. Batalden, M.D.; Karen Homa, MS; Marjorie Godfrey, MS RN; Christine Campbell; Linda Headrick, MD, MS, Thomas Huber, MS; Julie Mohr MSPH, PhD; John Wasson, MD: “ Microsystems in Health Care: Creating a Rich Information Environment.” The Joint Commission Journal on Quality Improvement, January 2003, Volume 29. • Eugene C. Nelson, D.Sc., M.P.H.; Paul B. Batalden, M.D.; Thomas P. Huber, M.S.; Marjorie M. Godfrey, M.S., R.N.; Linda A. Headrick, M.D.; Julie J. Mohr, Ph.D.; M.S.P.H.; John H. Wasson, M.D.; “ Microsystems in Health Care: Learning from High-Performing Front-Line Clinical Units.” The Joint Commission Journal on Quality Improvement, September 2002, Volume 28. • Godfrey M, Wasson J, Nelson E, Batalden P, Mohr J, Huber T, Headrick L.; “Clinical Microsystem Action Guide – Improving Health Care by Improving Your Microsystem”, Version 1.1: November 2001. • Clinical Microsystems provides an on-line version of the Clinical Action Guide. Hanover, NH: Health Care Improvement and Leadership Development at Dartmouth College. (See Clinicalmicrosystems.org)
If you want to learn more . . . References • Langley GJ, et al.: The Improvement Guide - A Practical Approach to Enhancing Organizational Performance. San Francisco: Jossey-Bass, 1996 • Nelson EC, Batalden PB, Ryer J: Clinical Improvement Action Guide, JCAHO, Oak Brook Terrace, IL, 1998. • Nelson EC, Wasson JH: "Using Patient-Based Information to Rapidly Redesign Care," Healthcare Forum Journal, 37(4):25-29, July/August 1994. • Quinn JB: Intelligent Enterprise: A Knowledge and Service Based Paradigm for Industry. New York, NY: The Free Press, 1992. • Rother M, Shook J: Learning to See: Value Stream Mapping to Add Value and Eliminate Muda. Brookline, MA: Lean Enterprise Institute, 1999. • Nelson EC, Splaine ME, Godfrey MM, Kahn V, Hess AR, Batalden PB, Plume SK: Using Data to Improve Medical Practice by Measuring Processes and Outcomes of Care. Joint Commission Journal on Quality Improvement, 26(12):667-685, December 2000. • Nelson EC, Batalden PB: Knowledge for Improvement: Improving Quality in the Micro-systems of Care. In: Goldfield N , Nash DB, eds. Managing Quality of Care in Cost-Focused Environment. Tampa, FL: Aspen Publishers; 1999:75-87.
If you want to learn more . . . References • Nelson EC, Batalden PB, Mohr JJ, Plume SK:Building A Quality Future. Frontiers of Health Services Management, 15(1):3-32, Fall 1998. • Batalden PB, Mohr JJ, Nelson EC, et al.: Continually Improving the Health and Value of Healthcare for a Population of Patients: The Panel Management Process. Quality Management in Healthcare, 5(3):41-51, Spring 1997. • Nelson EC, Mohr JJ, Batalden PB, Plume SK:Improving Health Care, Part 1: The Clinical Value Compass. The Joint Commission Journal on Quality Improvement, 22(4):243-258, April 1996. • Nelson EC, Batalden PB, Plume SK, Mihevc NT, Swartz WG:Report Cards or Instrument Panels: Who Needs What? The Joint Commission Journal on Quality Improvement,21(4):155-166, April 1995. • Weinstein JN, Brown PW, Hanscom B, Walsh T, Nelson EC: Designing an Ambulatory Clinical Practice for Outcomes Improvement: From Vision to Reality - The Spine Center at Dartmouth-Hitchcock, Year One. Quality Management in Health Care, 8(2):1-20, Winter 2000.