Download
1 / 1
10 likes | 97 Views
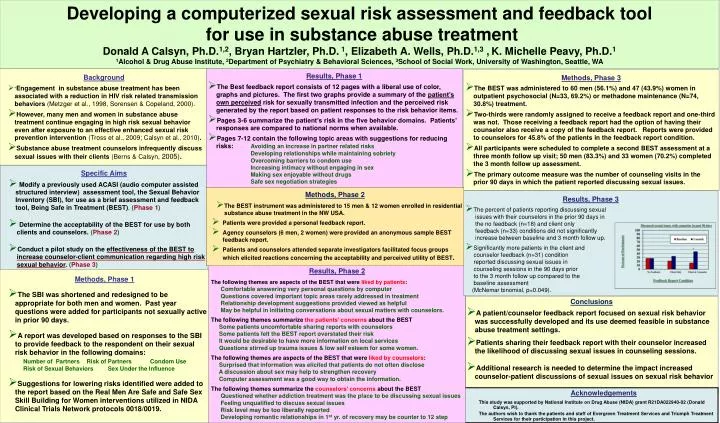
Developing a computerized sexual risk assessment and feedback tool for use in substance abuse treatment Donald A Calsyn, Ph.D. 1,2 , Bryan Hartzler, Ph.D. 1 , Elizabeth A. Wells, Ph.D. 1,3 , K. Michelle Peavy, Ph.D. 1

E N D
Developing a computerized sexual risk assessment and feedback tool for use in substance abuse treatment Donald A Calsyn, Ph.D.1,2, Bryan Hartzler, Ph.D. 1, Elizabeth A. Wells, Ph.D.1,3 ,K. Michelle Peavy, Ph.D.1 1Alcohol & Drug Abuse Institute, 2Department of Psychiatry & Behavioral Sciences, 3School of Social Work, University of Washington, Seattle, WA • Results, Phase 1 • The Best feedback report consists of 12 pages with a liberal use of color, graphs and pictures. The first two graphs provide a summary of the patient’s own perceived risk for sexually transmitted infection and the perceived risk generated by the report based on patient responses to the risk behavior items. • Pages 3-6 summarize the patient’s risk in the five behavior domains. Patients’ responses are compared to national norms when available. • Pages 7-12 contain the following topic areas with suggestions for reducing risks: Avoiding an increase in partner related risks • Developing relationships while maintaining sobriety • Overcoming barriers to condom use • Increasing intimacy without engaging in sex • Making sex enjoyable without drugs • Safe sex negotiation strategies • Background • “Engagement in substance abuse treatment has been associated with a reduction in HIV risk related transmission behaviors (Metzger et al., 1998, Sorensen & Copeland, 2000). • However, many men and women in substance abuse treatment continue engaging in high risk sexual behavior even after exposure to an effective enhanced sexual risk prevention intervention (Tross et al., 2009; Calsyn et al., 2010). • Substance abuse treatment counselors infrequently discuss sexual issues with their clients (Berns & Calsyn, 2005). • Methods, Phase 3 • The BEST was administered to 60 men (56.1%) and 47 (43.9%) women in outpatient psychosocial (N=33, 69.2%) or methadone maintenance (N=74, 30.8%) treatment. • Two-thirds were randomly assigned to receive a feedback report and one-third was not. Those receiving a feedback report had the option of having their counselor also receive a copy of the feedback report. Reports were provided to counselors for 45.8% of the patients in the feedback report condition. • All participants were scheduled to complete a second BEST assessment at a three month follow up visit; 50 men (83.3%) and 33 women (70.2%) completed the 3 month follow up assessment. • The primary outcome measure was the number of counseling visits in the prior 90 days in which the patient reported discussing sexual issues. • Specific Aims • Modify a previously used ACASI (audio computer assisted structured interview) assessment tool, the Sexual Behavior Inventory (SBI), for use as a brief assessment and feedback tool, Being Safe in Treatment (BEST). (Phase 1) • Determine the acceptability of the BEST for use by both clients and counselors.(Phase 2) • Conduct a pilot study on the effectiveness of the BEST to increase counselor-client communication regarding high risk sexual behavior.(Phase 3) • Methods, Phase 2 • The BEST instrument was administered to 15 men & 12 women enrolled in residential substance abuse treatment in the NW USA. • Patients were provided a personal feedback report. • Agency counselors (6 men, 2 women) were provided an anonymous sample BEST feedback report. • Patients and counselors attended separate investigators facilitated focus groups which elicited reactions concerning the acceptability and perceived utility of BEST. • Methods, Phase 2 • The BEST instrument was administered to 15 men & 12 women enrolled in residential substance abuse treatment in the NW USA. • Patients were provided a personal feedback report. • Agency counselors (6 men, 2 women) were provided an anonymous sample BEST feedback report. • Patients and counselors attended separate investigators facilitated focus groups which elicited reactions concerning the acceptability and perceived utility of BEST. • Results, Phase 3 • The percent of patients reporting discussing sexual • issues with their counselors in the prior 90 days in • the no feedback (n=18) and client only • feedback (n=33) conditions did not significantly • increase between baseline and 3 month follow up. • Significantly more patients in the client and • counselor feedback (n=31) condition • reported discussing sexual issues in • counseling sessions in the 90 days prior • to the 3 month follow up compared to the • baseline assessment • (McNemar binomial, p=0.049). Results, Phase 2 The following themes are aspects of the BEST that were liked by patients: Comfortable answering very personal questions by computer Questions covered important topic areas rarely addressed in treatment Relationship development suggestions provided viewed as helpful May be helpful in initiating conversations about sexual matters with counselors. The following themes summarize the patients’ concerns about the BEST Some patients uncomfortable sharing reports with counselors Some patients felt the BEST report overstated their risk It would be desirable to have more information on local services Questions stirred up trauma issues & low self esteem for some women. The following themes are aspects of the BEST that were liked by counselors: Surprised that information was elicited that patients do not often disclose A discussion about sex may help to strengthen recovery Computer assessment was a good way to obtain the information. The following themes summarize the counselors’ concerns about the BEST Questioned whether addiction treatment was the place to be discussing sexual issues Feeling unqualified to discuss sexual issues Risk level may be too liberally reported Developing romantic relationships in 1st yr. of recovery may be counter to 12 step • Methods, Phase 1 • The SBI was shortened and redesigned to be appropriate for both men and women. Past year questions were added for participants not sexually active in prior 90 days. • A report was developed based on responses to the SBI to provide feedback to the respondent on their sexual risk behavior in the following domains:Number of Partners Risk of Partners Condom Use • Risk of Sexual Behaviors Sex Under the Influence • Suggestions for lowering risks identified were added to the report based on the Real Men Are Safe and Safe Sex Skill Building for Women interventions utilized in NIDA Clinical Trials Network protocols 0018/0019. • Conclusions • A patient/counselor feedback report focused on sexual risk behavior was successfully developed and its use deemed feasible in substance abuse treatment settings. • Patients sharing their feedback report with their counselor increased the likelihood of discussing sexual issues in counseling sessions. • Additional research is needed to determine the impact increased counselor-patient discussions of sexual issues on sexual risk behavior Acknowledgements This study was supported by National Institute on Drug Abuse (NIDA) grant R21DA022940-02(Donald Calsyn, PI). The authors wish to thank the patients and staff of Evergreen Treatment Services and Triumph Treatment Services for their participation in this project.




![Specific Aims Workshop [NAME ] [“TITLE”]](https://cdn5.slideserve.com/9671983/specific-aims-workshop-name-title-dt.jpg)