Download
1 / 24
270 likes | 622 Views
Cardiac output (CO) and systemic vascular resistance (SVR)– the next vital signs?. Tom Archer, MD, MBA UCSD Anesthesia October 4, 2010. Blood pressure, while important, does not tell the whole story about health of the circulation. CO and SVR are important too. “Normal BP” =.

E N D
Cardiac output (CO) and systemic vascular resistance (SVR)– the next vital signs? Tom Archer, MD, MBA UCSD Anesthesia October 4, 2010
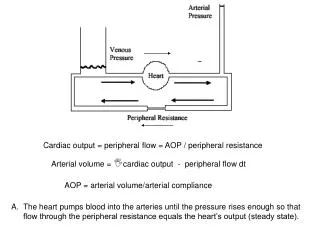
Blood pressure, while important, does not tell the whole story about health of the circulation. CO and SVR are important too. “Normal BP” = High SVR x Low CO (e.g. Hemorrhagic or cardiogenic shock) Low SVR x High CO (e.g. Sepsis) “Normal BP” = “Normal BP” = Normal SVR x Normal CO (e.g. Healthy person)
What if we could easily measure CO and SVR? • Assist both intensive and general medical care? • Fine tune medications (e.g. antihypertensives)? • Detect and monitor disease (e.g. pre-eclampsia, heart failure, sepsis, hemorrhage)? • Encourage healthy life style (diet, weight loss, exercise)?
Conditions decreasing SVR directly: • Anemia (viscosity is component of resistance) • Fever, hyperthyroidism (increased O2 demand) • Sepsis • Anaphylaxis • Neuraxial and other anesthetics
Conditions increasing SVR directly: • Severe pre-eclampsia • Essential hypertension? • Diabetes? • Smoking? • Obesity?
Conditions decreasing CO directly: • Heart failure or cardiogenic shock (MI, tamponade, cardiomyopathy, bradyarrythmia) • SVR increases in compensation for decreased CO in attempt to maintain BP.
Conditions increasing CO directly: • Pain, fear? • However– increased CO requires increased venous return. • Healthy heart pumps out what it receives (Frank-Starling mechanism). • Heart can be seen as “passive” servant of periphery!
In anesthesia we are often “cardiocentric” in thinking about CO • Emphasis is on stroke volume and heart rate. • Preload, contractile state and afterload. • Is the heart appropriately contractile and full? • Do we sometimes forget SVR?
Resistance arterioles also merit attention! • How much blood flow are the tissues demanding? • Is the tone of the resistance arterioles and capacitance veins appropriate for health? • What is the state of the endothelium of the resistance arterioles?
Are the resistance arterioles “misbehaving”? • Excessive tone: pre-eclampsia, essential hypertension? • Deficient tone: sepsis, anaphylaxis, neuraxial block.
Blood vessels Heart In health and disease, heart and blood vessels work together– the function of one affects the function of the other. Independent assessment of CO and SVR might be helpful in clarifying the relationship of heart, resistance arterioles and capacitance veins.
Blood vessels affect SVR and CO Heart affects CO and SVR Sick heart (cardiogenic shock) produces low CO and compensatory high SVR. Sick arterioles (sepsis) produces low SVR and compensatory high CO.
Methods for estimating CO and SVR • PA catheter (thermodilution or Fick)—highly invasive, but a gold standard. Can be continuous. • Echocardiography (TEE or TTE)—a minimally or non-invasive “gold standard”. TEE difficult on non-intubated patients. Requires training, labor-intensive, not continuous. Uses velocity time integral (VTI) to calculate “stroke distance” or compares diastolic and systolic LV areas to calculate “stroke area”.
End-diastolic area - End-systolic area = “stroke area” in one MRI slice. Same idea applies to echocardiography for calculation of stroke volume. David K. Shelton, Fundamentals of Diagnostic Radiology 3rd edition, 2007
Methods for estimating CO and SVR • VTI variants (Cardio-Q, USCOM). • Ultrasound measures blood flow duration and velocity in abdominal (Cardio-Q) or thoracic aorta (USCOM). Labor intensive, non-continuous and operator dependent.
Velocity-time integral (VTI) = “stroke distance” (SD). SD x aortic diameter = stroke volume (USCOM advertisement).
Methods for estimating CO and SVR • Pulse contour analysis (Vigileo, LiDCO). • Stroke volume from contour of the pulse. Requires arterial line, “minimally invasive”. Continuous, operator independent, makes many assumptions. Best for “trend following”?
Oxytocin bolus decreases SVR and increases CO at cesarean delivery (data from LiDCO pulse contour analysis) Archer TL et al. International Journal of Obstetric Anesthesia (2008) 17, 247–254
Impedance cardiography (IC) • Non-invasive and continuous. Little training required. “Hands-free”. • Long history (NASA, 1960’s) and multiple iterations and algorithms. • Bo-Med, Cardiodynamics, Cheetah, Cardiotronic). • All look at same signal but interpret it in different ways.
All IC systems work with the same signal– but process it differently. Processing algorithms are patented “intellectual property”. Bo-Med and Cardiodynamics work with impedance change during systole (-dZ(t). Cheetah and Cardiotronic work with rate of impedance change during systole dZ(t)/dt. C. Schmidt et al British Journal of Anaesthesia 95 (5): 603–10 (2005)
Cardiac and stroke indices increase with uterine contractions 8 CI 3 90 SI 40 100 HR 80 0 15 30 Minutes Archer TL and Shapiro A, UCSD, unpublished
In severe pre-eclampsia, MgSO4 and labetalol decrease SVR and increase CO (data from Aesculon electrical velocimetry) Archer TL, Conrad B. International Journal of Obstetric Anesthesia, In Press
What about CVP? • (MAP – CVP) = CO x SVR • Since CVP is usually much less than MAP, we may be able to ignore or estimate the CVP value and still get clinically useful estimates for SVR. • So, MAP (approximately) = CO x SVR.
Summary • Currently, measurement of CO and SVR can be labor-intensive, invasive, risky, uncomfortable and non-continuous. • Easy, painless, non-invasive and continuous estimation of CO and SVR might improve care of multiple conditions affecting the heart, resistance arterioles and capacitance veins. • CO and SVR might be the next vital signs.