Download
1 / 23
230 likes | 437 Views
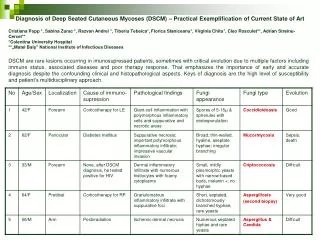
Case 1. A Quick Vindicates (insert groan here) of Back Pain. Vascular AAA Aortic dissection Avascular necrosis -> pathological fracture Infective Osteomyelitis TB All can cause pathological fractures Idiopathic Paget’s disease Neoplastic

E N D
A Quick Vindicates (insert groan here) of Back Pain • Vascular • AAA • Aortic dissection • Avascular necrosis -> pathological fracture • Infective • Osteomyelitis • TB • All can cause pathological fractures • Idiopathic • Paget’s disease • Neoplastic • Primary, mets, haematological -> pathological fractures • Degenerative • Osteoarthritis • Spinal stenosis • Disk prolapse • Inflammatory • Ankylosing spondylitis, psoriatic arthritis, Reactive arthritis (Hx separates these conditions) • Congenital • Kyphoscoliosis • Spondylolisthesis • Spina bifida • Autoimmune • Lupus • Trauma • Muscle tears • Ligament tears • Joint strain, rupture • Vertebral fractures • Endocrine/Metabolic • Cushing's, corticosteroids • Pathological fractures: osteoporosis, osteomalacia, Paget’s, hyperparathyroidism, • Social • Worker’s compensation claim • Somatisation
The Case - Michael • Michael, 24YO male presented 1 week ago with a red eye, possibly related to long standing back pain, resolved by topical corticosteroids. • Progressively worsening back pain began at 16YO, described as aching of buttocks and lower back with stiffness that is worse in the morning • Pain is worse at night, occasionally waking him, and relieved by gently daily activityand NSAIDS
Which of these Correlates to Michael’s Back Pain? • Age: Pain began at 16YO so osteoarthritis, spinal stenosis, Paget’s and malignancy are less likely • Character/duration/intensity: Long standing worsening ache makes muscle strain, traumatic fracture, infection less likely. Not resolving within 6-8 weeks and no leg pain, paraesthesia makes disk herniation less likely. • Vertebral vertebral misalignment (spondylolisthesis, kyphoscoliosis) still possible • Aching pain of buttocks and lumbosacral region worsening at night, morning stiffness, improved by exercise, <40YO, NSAID responsive, uveitis all point to ankylosing spondylitis (70% S/S U.T.D)
Ankylosing Spondylitis • Sacral-iliac joint (sacroiliitis) is the main location of disease, being precocious affected and is characterized by the presence of subchondral granulation tissue, which leads to cartilage erosion of the iliac and sacred cartilage. Subsequently, occurs the replacement of granulation tissue with regenerative fibro-cartilage, followed by the ossification of the joint; • The joints of the spine: first, there is an inflammatory granulation tissue, located in the insertion of the fibrous ring of inter-vertebral disc, on the edge of inter-vertebral body. The edges of the vertebral body and the peripheral region of fiber ring will be eroded and then will calcify, creating the syndesmophyte; • Anterior inter-vertebral ligament is suffering a process of inflammation, then will appear fibrosis and finally will be calcified; • Peripheral joints (hip, shoulder, knee) are less interested; • The eye is affected at 20% -35% of patients with the appearance of irides inflammation and iridocilities; • The heart: aortic valve thickening and fibrosis of excito-conductive system; • Renal damage, more rare, it is represented by nephropathy with immunoglobulin A
What Specific Focussed Questions May Help Clarify the Diagnosis? • Do you suffer from diarrhoea or bloody diarrhoea? Has anyone in your family suffered from and inflammatory bowel disorder? • Do you have limited movement of the lower back? • Are you getting more out of breath too easily? • What other joints, if any, are affected? • Do you have a painful Achilles tendon? • Is there a Hx of back pain associated with trauma? • Is there a Hx of GI infections? • Sexual Hx focussing on STI’s and unsafe sexual practices? • Do you or your family have psoriasis, IBD, RA? CIGS?
What group of disorders is this man's diagnosis likely to fit into? • Diseases belonging to the seronegative spondyloarthropathies' group include ankylosing spondylitis, Reiter syndrome, enterohepatic arthritis, psoriatic arthritis
Reactive Arthritis • Reactive arthritis is a post infectious arthritis caused by Chlamydia, Yersinia, Salmonella, Campylobacter, Shigella infections of the GI tract and STI’scausing asymmetric oligoarthritis, commonly affecting the knees but can cause lower back and buttock pain and arthritis of the upper extremities and small joints • Ocular inflammation and uveitis is common
Reactive Arthritis • Also causes enthesitis: pain in the plantar fascia, especially under the heel • Dactylitis: swollen sausage shaped digits
Psoriatic Arthritis • Distal arthritis, assymetric and symmetric oligo and polyarthritis, enthesitis and dactylitis • Associated with skin and/or nail psoriasis with the severity of nail involvement reflects severity of joint involvement. • In 13-17% the arthritis presents prior to skin lesions and in this case the presence of onycholysis, distal joint involvement with asymmetric distribution differentiates it from other forms. • Ocular inflammation and uveitis is common
Enterohepatic Arthritis • Associated with IBD (1 in 5 with UC or Crohns will develop this) • Mainly affects peripheral limb joints and spondylarthropathy • Ocular inflammation and uveitis is common
What is the incidence for this condition? - How does this compare to RA? • Prevalence: • 0.1% to 1.4% depending on the population studied • 5% to 6% in HLA-B27–positive persons • Ankylosing spondylitis is found to be the aetiology of chronic low back pain in 4% to 5% of patients • RA • Incidence: • Women: 53/100,000 • Men: 28/100,000 • Incidence of RA increases from young adulthood to age 75 (14/100,000 to 104/100,000 in women and 4/100,000 to 72/100,000 in men) • Although the incidence declined during the 1985-1994 period and previous intervals, it increased again in the 1995-2007 period • Prevalence: • Women: 1% • Men: 0.4% • Lifetime risk: • Women: 3.6% • Men: 1.7%
Is there relevance in the family history aspects of his story? • An individual's risk of developing AS is increased 5.6- to 16-fold if there is a first degree relative with AS. This risk depends partly upon the presence of HLA-B27: 10 to 20 percent of HLA-B27 positive individuals with affected first degree relatives develop AS
What are the range of clinical symptoms and signs in these patients? • The clinical features of AS can be divided into those that arise from: • Spinal and sacroiliac involvement • Hip and shoulder ("root" joint) involvement • Costovertebral, manubriosternal, sternoclavicular, and costochondral inflammation • Inflammation of extraspinal entheses • Peripheral arthritis • Other (extraarticular) organ involvement • Low back pain 75% of patients present with this first. “Inflammatory back pain” is different to “mechanical back pain”. Inflammatory back pain improves with exercise but not with rest and occurs at night. • Dyspnea due to involvement of the thoracic region causing decreased chest expansion • Constitutional symptoms such as fatigue, weight loss, and low-grade fever • Asymmetric tenderness, swelling, erythema, and decreased range of motion of one or more peripheral joints, usually large axial joints (hips and shoulders) and more commonly in the lower extremities
Why is diagnosis often delayed from presentation? • AS is a disease of often insidious onset. The plain film radiologic diagnosis is somewhat observer-dependent. In addition, patients with milder disease and involvement of peripheral joints may have been misdiagnosed as seronegative rheumatoid arthritis. • There are no formal diagnostic criteria for AS, but there are several sets of classification criteria that identify the features that are important in making the diagnosis.
What tests would you expect a rheumatologist to perform and what results would be confirmatory of your primary diagnosis? • An assessment of the C-reactive protein (CRP) and determination of the presence or absence of HLA-B27, particularly among Caucasian patients, are very useful and should be carried out in all patients. • A therapeutic trial of a nonsteroidal antiinflammatory drug (NSAID) is very useful in the diagnosis of axial spondyloarthropathy (SpA). • An abnormal appearing sacroiliac (SI) joint on plain radiographs is a hallmark of longstanding AS.
What are the treatment options for this condition? • The goals of treatment are to reduce pain and stiffness, preserve or restore function, prevent damage and deformity, maintain posture, slow disease progression, and minimize the impact of extraspinal and extra-articular manifestations. • NSAIDs should be prescribed as initial therapy to relieve the pain associated with ankylosing spondylitis • A tumor necrosis factor (TNF)–α inhibitor (eg, etanercept, infliximab, adalimumab, golimumab) should be prescribed for patients with axial disease that does not respond to NSAID therapy. • Methotrexate has not been shown to be effective in clinical trials for either the axial or appendicular manifestations of ankylosing spondylitis. However, it can be considered as an alternative for patients with predominantly axial disease who either cannot obtain or cannot tolerate a TNF-α inhibitor. • Local injections of a corticosteroid (eg, triamcinolone, methylprednisolone) into joints or entheses may be effective for symptomatic relief, but long-term use is associated with adverse effects.