Download
1 / 30
310 likes | 567 Views
Proprioceptive training. Dr. Ali Abd El-Monsif Thabet. Proprioceptive system: A general term used to cover all those sensory systems that are involved in providing information about position, location, orientation and movement of the body and its parts (sensing position and motion of the body).

E N D
Proprioceptive training Dr. Ali Abd El-Monsif Thabet
Proprioceptive system: A general term used to cover all those sensory systems that are involved in providing information about position, location, orientation and movement of the body and its parts (sensing position and motion of the body).
Ruffini ending Pacinian corpuscle Fig. 3 a. Ruffini endings b. Pacinian corpuscle
Cutaneous mechanoreceptors Cutaneous mechanoreceptors are located in the skin By morphology Ruffini's end organ detects sustained pressure. Meissner's corpuscle detects changes in texture (vibrations around 50 Hz); Pacinian corpuscle detects deep pressure and rapid vibrations (about 200-300 Hz). Merkel's disc detects sustained touch and pressure. Free nerve endings (touch, pressure, stretch) Hair folliclesreceptors are located in hair follicles and sense the position
AFFERENT INPUT LEVELS OF MOTOR CONTROL • Peripheral afferents • joint • muscle • skin Spinal reflexes Cognitive programming CNS MUSCLE Visual receptors Brain Stem balance Vestibular receptors
Purposes of proprioception: 1- Provide awareness of position sense and kinesthesia. 2- Produce coordinated reflex effects on muscle tone and balance. 3- Provide peripheral feedback so the CNS can design and modify effective motor programs
Measurement Methods Proprioceptive assessment tests: 1. Tests of angular reproduction (AR) 2.Threshold to detect passive movement (TTDPM)
Indications for proprioceptive training 1-Joint sprain or strain 2-Joint instability (shoulder dislocation ,ligament laxity or weakness) 4-Athletic protection against reinjury
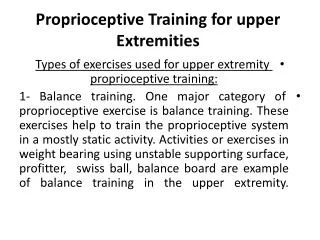
Proprioceptive Training Proprioceptive exercises The objective of kinesthetic and proprioceptive training is to restore the neurosensory properties of injured capsuloligamentous structures and enhance the sensitivity of uninvolved peripheral afferents. Rehabilitation programs begin with restoration of range of motion, muscular endurance, and muscular strength. These exercises, in a nonspecific fashion, stimulate joint and muscle proprioceptors in the injured extremity Joint compression is believed to maximally stimulate articular receptors and can be accomplished with closed chain exercises throughout the available ROM. Early joint repositioning tasks enhance conscious proprioceptive and kinesthetic awareness, eventual leading to unconscious appreciation of joint motion and position. Applying elastic bandage can provide additional proprioceptive and kinesthetic formation by stimulating cutaneous receptors
Proprioceptive Training General principles 1- Balance is achieved first, then coordination, then agility ( the ability to control the direction of a body or its parts during rapid movement, it requires flexibility, strength, power, speed, balance, and coordination and involves rapid change of direction and sudden stopping and starting). 2- Exercises progress from simple to complex . 3- Initial exercises are performed slowly and perfomed in controlled situations
Proprioceptive Training 4- Advancement is made only after the activity is mastered 5- Progression is to more complex activities and evolves to specific performance activities: Make activity more complex Perform simple activity at a faster pace Require a more powerful output Have patient perform more than one task simultaneously 6 - Goal: perform the activity accurately: Do difficult proprioceptive activities early in exercise session so patient not as fatigued Repetition
Figure 8 : Left, Eyes open, Fitter balance in push-up position with platform rocking in the frontal plane. Right, Fitter balance in push up position with platform rocking in the sagittal plane.
Figure 9 : Eyes open, Gymnastic ball balance feet-elevated position
Figure 11 : Dynamic shoulder stabilization in all four position but with one hand on a wobble board and the other hand held off the floor. The shoulder girdle is challenged as the patient tries to keep the edge of the wobble board from touching the floor.
Fig. 12 Dynamic stabilization exercises for the upper extremity. A, Push-ups. B, Horizontal abduction on a slide board
Fig. 14 Active and passive repositioning activities should be performed in functional positions specific to individual sports.