Download
1 / 12
120 likes | 307 Views
West Suffolk Hospitals NHS Trust. Report To: Trust Board Date: December 2009 Title: Quality Report Report of: Nichole Day, Executive Chief Nurse. Summary:

E N D
West Suffolk Hospitals NHS Trust Report To: Trust Board Date: December 2009 Title: Quality Report Report of: Nichole Day, Executive Chief Nurse
Summary: This report provides the Board with information to assess the Trust’s performance against quality indicators, including patient experience, clinical outcomes and effectiveness, and patient safety. The report has been revised and is presented in a new format with new indicators/measures that take into account the requirements of CQUIN, priorities identified in the Quality Accounts, and workstreams within the Trust such as the Patient Safety First Initiative. Some of the new indicators are in the development stage, with targets and data collection processes currently being agreed, the detail for these will therefore be added into the report in due course. Recommendation: The Board is asked to receive and note the contents of this report. Controls Assurance Reference:To Achieve performance levels in accordance with the CQC “Standards for Better Health”
Contents • Key Performance Indicator Dashboard • Introduction • Outcomes and Effectiveness • Patient Safety • Patient Experience • Conclusion
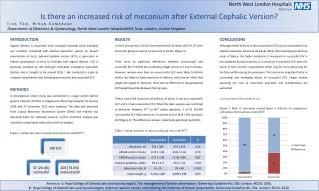
2. Introduction Introduction: This report provides the Board with information on our performance in relation to the key quality indicators. Detail is provided on those indicators that are traffic lighted amber or red or require a fuller explanation.
3. Outcomes and Effectiveness • Hospital Standardised Mortality Ratio • The graph demonstrates that overall HSMR for the West Suffolk Hospital is below that which would be expected given our patient mix. • Pain management • This indicator reports on whether pain was assessed at every set of patient observations. A baseline audit was carried out in the second quarter of the year and repeated last month. This has been the focus of attention for some time in Surgery (where the pain specialist nurses provide input and advice) but has not had the same emphasis in medicine where specialist nurse input is limited. This audit also includes midwifery where pain is managed but assessment has not been routinely documented. The results show a 40% compliance at the baseline audit rising to 49% in the second audit. There is a large degree of variability from area to area. For example medicine had no compliance in the baseline audit, this increased to 29% in the second audit. The Specialist Nurse team are currently providing training on pain assessment to the medical wards and looking at the introduction of a pain assessment tool that is suitable for use with patients with learning disabilities and dementia. Compliance in surgery was higher at the first audit and rose by 20% in the second audit.
3. Outcomes and Effectiveness Clostridium difficile The graph demonstrates that we are well below trajectory for the first six months of the year. MRSA bacteraemias We are below trajectory for the year to date with no new hospital acquired MRSA bacteraemias this month. Compliance with peripheral cannula and urinary catheter HI actions remains high.
4. Patient Safety Patient Falls A similar number of falls and fallers as last month. A new post fall action plan is being piloted on the three wards with the largest number of falls and a specific action plan for reducing falls and dealing with recruitment issues has been agreed for one of these wards with staffing issues. Pressure ulcers No hospital acquired grade 3 or 4 pressures ulcers since April. A slight rise this month in ward acquired pressure ulcers but this includes a small number of patients who were on the Liverpool care pathway and refused to be moved.
4. Patient Safety • Patient Safety Walkabouts • The Walkabouts have now visited both medical and surgical wards and have engaged with the porters and the medical secretaries. • The themes remain as previously indicated and continue to warrant specific actions at the individual, ward and corporate level. • Actions from the previous quality reports are ongoing including • The purchasing and distribution of underwire bed ties across the Trust to prevent falls. • Improvements in the hand over system in use for patients being transferred from ward to ward. • The review of patient’s mobility throughout the hospital when requiring oxygen. • Develop Trust wide reporting of numbers of patients who are transferred to or from wards after 22.00 hours and before 08.00 hours • Considering the development of a library of non electrical equipment. • This month, actions for consideration have included • Individual: • Increasing the awareness of WSH staff to departmental roles eg porters, housekeepers, governance department through the Green Sheet. • Establish current practices re oxygen cylinder management and the facilities for their storage. • Ward • Revisit information handover from staff to porters regarding patient mobility to release time to care. • To provide appropriate information resources to the ward (F4) regarding the need to remain seated after knee/hip operations such as laminated poster sheets and wall posters. • To ensure effective communication between consultants and junior doctors in timely medication prescribing and discharge planning. • To ensure robust processes around nutritional management for patients considered for alternative means of nutrition. • Corporate • At a corporate level call bells remain a priority for staff. • Global Trigger Tool • A new Consultant is taking over the audit for the global trigger tool and this month training of the Consultant has taken place. No results are therefore reported this month
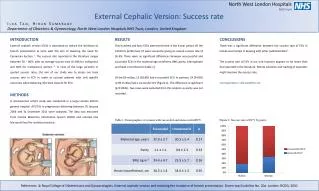
5. Patient Experience 5.1 Patient Satisfaction (Near patient TV) Satisfaction has increased slightly from 79% to 82% despite three new questions being added to the survey that did not produce high results. The questions added were related to single sex accommodation and response to call bells. Some patients reported non-segregated toilet/washing facilities despite this being in place on all wards, and even some of those on wards F7 and F8 which are single sex wards reported sharing facilities with the opposite sex. 5.2 Patient Satisfaction (PET) Responses using the PET continue at high levels. Satisfaction has increased overall this month. Perception of cleanliness in PAU has improved since the replacement of the flooring and chairs in the waiting area. Patients being told about delays is the other main area for improvement and as reported last month an action plan is in place to address this issue.
5. Patient Experience 5.3 Environment and cleanliness Cleanliness improved to 91% this month. 5.4 Hand Hygiene Compliance with hand hygiene and bare below the elbows was 99%.
6. Conclusion • The Trust is performing well with regard to clinical outcome measures including infection control. • A greater emphasis is needed on the documentation of pain assessment. This is being taken forward by the Pain Management Specialist Nurse Team. • Cleanliness levels have improved this month and should be maintained due to a successful recruitment campaign.