Download
1 / 17
170 likes | 384 Views
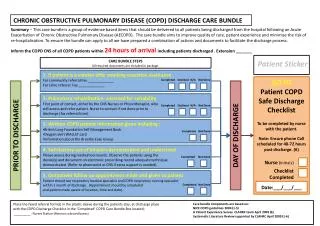
COPD (Chronic Obstructive Pulmonary Disease). Dr. Meg- angela Christi Amores. COPD. Global Initiative for Chronic Obstructive Lung Disease (GOLD) a disease state characterized by airflow limitation that is not fully reversible Includes:

E N D
COPD(Chronic Obstructive Pulmonary Disease) Dr. Meg-angela Christi Amores
COPD • Global Initiative for Chronic Obstructive Lung Disease (GOLD) • a disease state characterized by airflow limitation that is not fully reversible • Includes: • emphysema, chronic bronchitis, and small airways disease
COPD • Emphysema • an anatomically defined condition characterized by destruction and enlargement of the lung alveoli • Chronic Bronchitis • a clinically defined condition with chronic cough and phlegm • Small airways disease • a condition in which small bronchioles are narrowed
Risk Factors • Cigarette Smoking • Intensity: pack years (sticks/day for years) • most highly significant predictor of FEV1 • Airway responsiveness • asthma, chronic bronchitis, and emphysema are variations of the same basic disease • Respiratory infections • Remains to be proven
Risk Factors • Occupational Exposures • general exposure to dust at work • coal mining, gold mining, and cotton textile dust • Ambient Air pollution • living in urban compared to rural areas • Remains to be proven • Passive, or Second-Hand, Smoking Exposure • Genetic Considerations
Natural History • Effect of cigarette smoking depends on intensity, timing during growth, basal function
Pathophysiology • Airflow obstruction • Determined by spirometry: FEV1 and FVC • chronically reduced ratio of FEV1/FVC • seldom shows large responses to inhaled bronchodilators • Hyperinflation • "air trapping“ • helps to compensate for airway obstruction
Pathophysiology • Gas Exchange • Nonuniform ventilation and ventilation-perfusion mismatching
Pathology • Large Airway • Cigarette smoking often results in mucous gland enlargement and goblet cell hyperplasia • proportional to cough and mucus production • Small Airways • major site of increased resistance in most individuals with COPD is in airways 2 mm diameter • goblet cell metaplasia and replacement of surfactant-secreting Clara cells with mucus-secreting and infiltrating mononuclear inflammatory cells
Pathology • Lung Parenchyma • destruction of gas-exchanging airspaces • walls become perforated and later obliterated with coalescence of small distinct airspaces into abnormal and much larger airspaces • Macrophages accumulate • Centriacinaremphysema- most frequently associated with cigarette smoking • Panacinaremphysema - usually observed in patients with alpha1AT deficiency
Clinical presentation • History • cough, sputum production, and exertionaldyspnea • exertionaldyspnea, often described as increased effort to breathe, heaviness, air hunger, or gasping, can be insidious • patient's ability to perform them has changed
Clinical presentation • Physical Findings • entirely normal physical examination – early • signs of active smoking, including an odor of smoke or nicotine staining of fingernails • prolonged expiratory phase and expiratory wheezing- more severe • signs of hyperinflation include a barrel chest and enlarged lung volumes
Laboratory Findings • hallmark of COPD is airflow obstruction • Pulmonary function testing shows airflow obstruction with a reduction in FEV1 and FEV1/FVC • lung volumes may increase
Treatment • SMOKING cessation • Bronchodilators • Anticholinergic agents • Beta agonists • Inhaled Glucocorticoids • Oral Glucocorticoids • Theophylline • Oxygen
Treatment • General Medical Care • Pulmonary Rehabilitation • Lung Volume Reduction Surgery • Lung Transplantation