Download
1 / 37
370 likes | 509 Views
M.E . Research and Practice conference at Hove Town Hall 7 October 2014 Slides from Dr Zoe Gotts’ presentation. Assessing & treating sleep disturbance in M.E./CFS M.E. Research & Practice 7 th October 2014. Dr Zoe Gotts Northumbria Centre for Sleep Research (NCSR).

E N D
M.E. Research and Practice conference at Hove Town Hall7 October 2014Slides from Dr Zoe Gotts’ presentation
Assessing & treating sleep disturbance in M.E./CFSM.E. Research & Practice7th October 2014 Dr Zoe Gotts Northumbria Centre for Sleep Research (NCSR) Northumbria Centre for Sleep Research
CFS/ME Research in the North East Northumbria Centre for Sleep Research • Exciting field to work in – research teams committed to engaging with patients • North East team of researchers & clinicians working together • Newcastle University Fatigue Research Centre • Wider research focus – researchers/clinicians outside of the field getting involved • Multidisciplinary collaboration • This is how the research is being driven (other Universities may follow suit…)
Working together… Northumbria Centre for Sleep Research - HPA axis - autonomic dysfunction - Immune system - neuropsychological performance - mitochondrial genomics - sleep - pain - muscles/physiotherapy - Investigating and managing fatigue • Newcastle University Fatigue Research Centre • Institute of Cellular Medicine • Institute of Neuroscience • Northumbria Centre for Sleep Research • CRESTA (Clinics for Research & Service in Themed Assessments) Researchers & clinicians working together to better understand the causes and impact of CFS/ME & to improve treatment Researchers and students in discussion at the research presentations
My PhDThe role of sleep in CFS/ME Northumbria Centre for Sleep Research • 3-year programme of research supported my Action for ME • UNN & NCL collaboration • Allowed me to focus in depth on one aspect of this condition – sleep • UK CMRC – invited to be a member of the exec board (early career researcher) Key research questions • what kinds of sleep abnormalities? • are these the same for all patients? • do these impact upon existing symptoms? • is it possible to assess sleep in a better way?
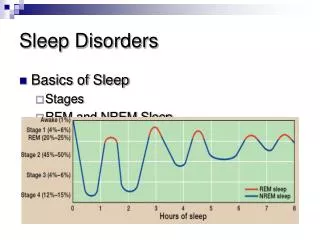
The role of sleep in CFS/ME Northumbria Centre for Sleep Research - early, middle, late insomnia. - reversed/irregular insomnia - oversleeping - frequent awakenings, - loss of restorative feelings. Some evidence of objective sleep abnormalities - but no consistent pattern! PSG, polysomnography *Rates from National Outcomes Database; 94% patients report disturbed sleep/unrefreshing sleep during assessment.
Northumbria Centre for Sleep Research Mixed methods approach • Qualitative Interviews with patients • Subjective sleep - 101 Sleep Diaries • Objective sleep - 343 Polysomnography (PSG) recordings • Detailed sleep assessment (feasibility) study
Qualitative Interviews Northumbria Centre for Sleep Research • Aim:Understand the extent to which sleep, its management & problems, are linked to the lived experience of ME/CFS & how it interacts with other symptoms. • No existing in-depth sleep-specific qualitative studies! • A good starting point in my research with ME/CFS patients • 11 Qualitative Interviews with ME/CFS patients • Face-to-face (patient’s home/university), telephone, Skype • Thematic analysis • Under review. . .
Qualitative Interviews Nature and frequency of sleep problems and factors that disturb sleep in the sample of patients (N = 11) SOL, sleep onset latency; WASO, wake after sleep onset
Qualitative Interviews Nature and frequency of sleep problems and factors that disturb sleep in the sample of patients (N = 11) SOL, sleep onset latency; WASO, wake after sleep onset
Variation between individuals Themes Variability over illness course Disturbers of sleep Sleep disturbances Maintenance/exacerbation of symptoms Balancing activity Effect on daytime functioning Attempts at coping & sleep management Adaptation & accepting disturbed sleep Impact on QOL and living Beliefs about impact on daytime functioning Alternative treatment approaches “ Sleep central to wellbeing… direct bearing on course & progression of illness ” Main themes & sub-themes elicited from patient narratives
Key message! Sleep disturbances were highly unpredictable and variable over time, but played a key role in symptom experience. Word cloud of Patient narratives
Subjective sleep(Diaries) • Aim: Examine subjective sleep quality in ME/CFS and its associations with key dimensions of the illness experience (fatigue, sleepiness, cognitive functioning, mood) • 101 patients (16-68 yrs, 81.2% female) • Standardised sleep diary over 14 days • Functional Assessments: • Fatigue (Chalder) • Sleepiness (ESS) • Cognitive functioning (CFQ, TMT) • Mood (HADS)
Subjective sleepMain Findings • Considerable variability in sleep characteristics across sample • 79.2 % patients napping during the day! (39.55±55.35 min) Mostly in the afternoon-evening period (31.74±43.94 min) • Total duration of daytime napping (particularly in the PM) had a negative impact on patients’ daytime cognitive functioning and levels of sleepiness • Shorter illness length & longer wake time (during sleep period) associated with more fatigue (adjustment?) Gotts, Z M, Ellis, J G, Brannan, K, Newton, J L, & Deary, V (2013). Daytime Napping Impairs Cognitive Functioning in Chronic Fatigue Syndrome (CFS). UK Society for Behavioural Medicine (UKSBM) 9th Annual Scientific Meeting, 9-10 December 2013, Oxford, p.76.
Objective sleep Aims: • Identify whether sleep-specific phenotypes exist in ME/CFS; 2. Explore objective characteristics that could differentiate phenotypes (whilst also being relevant to routine clinical practice) • Secondary analysis of existing PSG data from fatigue clinic in Holland • 343 (single-night) PSG recordings • Largest ME/CFS PSG dataset to date! Gotts Z M, Deary V, Newton J L, Van der Dussen D, De Roy P, & Ellis J G (2013). Are there sleep-specific phenotypes in patients with chronic fatigue syndrome? A cross-sectional polysomnography analysis. BMJ Open, 3(6).
343 First-night single PSGs performed on a sample of referrals to a fatigue service 101 Suspected Apnoea* (AHI>15) 239 Unexplained 17 Suspected PLMs* (PLMI>5) 30% Primary Sleep Disorder Figure 1: Study Overview *AASM, American Academy of Sleep Medicine. PLM, periodic leg movement
343 First-night single PSGs performed on a sample of referrals to a fatigue service 101 Suspected Apnoea* (AHI>15) 239 Unexplained 17 Suspected PLMs* (PLMI>5) Age = 34.4 (SD 11.84) Sex = 210 (87.9%) Female BMI = 23.54 (SD 4.26) AHI = 4.5 (SD 4.11) PLM Index = 1.01 (SD 0.9) TST = 435.22 (SD 242.65) WAKE TIME = 85.78 (SD 64.44) SEI = 83.04 (SD 13.04) SL = 28.05 (SD 30.31) WASO = 57.44 (SD 62.46) Number of Awakenings = 11.82 (SD 8.48) Number of Arousals per/hour = 6.64 (SD 16.01) %N1 of TST = 15.10 (SD 11.81) %N2 of TST = 37.74 (SD 12.60) %N3 of TST = 32.11 (SD 13.44) %REM of TST = 15.32 (SD 6.41) REM Latency = 65.19 (87.35) Sleep profile highly variable indicating presence of phenotypes Figure 1: Study Overview
343 First-night single PSGs performed on a sample of referrals to a fatigue service 101 Suspected Apnoea* (AHI>15) 239 Unexplained 17 Suspected PLMs* (PLMI>5) Age = 34.4 (SD 11.84) Sex = 210 (87.9%) Female BMI = 23.54 (SD 4.26) AHI = 4.5 (SD 4.11) PLM Index = 1.01 (SD 0.9) TST = 435.22 (SD 242.65) WAKE TIME = 85.78 (SD 64.44) SEI = 83.04 (SD 13.04) SL = 28.05 (SD 30.31) WASO = 57.44 (SD 62.46) Number of Awakenings = 11.82 (SD 8.48) Number of Arousals per/hour = 6.64 (SD 16.01) %N1 of TST = 15.10 (SD 11.81) %N2 of TST = 37.74 (SD 12.60) %N3 of TST = 32.11 (SD 13.44) %REM of TST = 15.32 (SD 6.41) REM Latency = 65.19 (87.35) WASO ≥30 min problematic (Edinger et al., 2004) Figure 1: Study Overview
343 First-night single PSGs performed on a sample of referrals to a fatigue service 101 Suspected Apnoea* (AHI>15) 239 Unexplained 17 Suspected PLMs* (PLMI>5) Age = 34.4 (SD 11.84) Sex = 210 (87.9%) Female BMI = 23.54 (SD 4.26) AHI = 4.5 (SD 4.11) PLM Index = 1.01 (SD 0.9) TST = 435.22 (SD 242.65) WAKE TIME = 85.78 (SD 64.44) SEI = 83.04 (SD 13.04) SL = 28.05 (SD 30.31) WASO = 57.44 (SD 62.46) Number of Awakenings = 11.82 (SD 8.48) Number of Arousals per/hour = 6.64 (SD 16.01) %N1 of TST = 15.10 (SD 11.81) %N2 of TST = 37.74 (SD 12.60) %N3 of TST = 32.11 (SD 13.44) %REM of TST = 15.32 (SD 6.41) REM Latency = 65.19 (87.35) Normal parameters N1: 2-5% N2: 45-55% N3: 13-23% REM: 20-25% (Carskadon & Dement, 2011) Confirms objective sleep difficulties in this sample! Figure 1: Study Overview
Cluster Analysis Iteration Process • 154 Groups in Primary (First-step) Iteration • 39 Groups in Second Iteration • 9 Groups in Third Iteration • 9 Groups in Fourth Iteration • 8 Groups in Fifth Iteration • 4 Groups in Sixth Iteration • 2 Groups in Seventh Iteration • 2 Groups in Eighth Iteration • 2 Groups in Ninth Iteration • 2 Groups in Tenth Iteration • 2 Groups in Eleventh Iteration • 2 Groups in Twelfth Iteration • 2 Groups in Thirteenth Iteration • 2 Groups in Fourteenth (Final) Iteration Retain minimum 5% of sample per group
Sleep Phenotypes Key Characteristics • Type 1 – Long sleep onset, few awakenings, normal quality (Sleep Onset Insomnia?) • Type 2 – Restless, high N2, arousals, normal quality (NRS) (pain patients/noise sensitivity?) • Type 3 – Few awakenings, lots of deep sleep (Hypersomnolence*?) • Type 4 – Lots of awakenings, short sleep duration (Sleep Maintenance Insomnia?) *The term Hypersomnolence will replace hypersomnia under the DSM-5
Sleep Phenotypes Length of illness? • Type 1 – Long sleep onset, few awakenings, normal quality (Sleep Onset Insomnia?) • Type 2 – Restless, high N2, arousals, normal quality (NRS) (pain patients/noise sensitivity?) • Type 3 – Few awakenings, lots of deep sleep (Hypersomnolence*?) • Type 4 – Lots of awakenings, short sleep duration (Sleep Maintenance Insomnia?) Patients may fall into more than one of these sleep-types - at different stages of their illness *The term Hypersomnolence will replace hypersomnia under the DSM-5
Sleep Phenotypes Importantly! Amenable to different kinds of treatment • Type 1 – Long sleep onset, few awakenings, normal quality (Sleep Onset Insomnia?) • Type 2 – Restless, high N2, arousals, normal quality (NRS) (pain patients/noise sensitivity?) • Type 3 – Few awakenings, lots of deep sleep (Hypersomnolence*?) • Type 4 – Lots of awakenings, short sleep duration (Sleep Maintenance Insomnia?) • Therapeutic / Pharmacological Interventions? • Standalone / adjunct? *The term Hypersomnolence will replace hypersomnia under the DSM-5
Northumbria Centre for Sleep Research Detailed Sleep Assessment: A feasibility study
Detailed Sleep Assessment • Aim: Determine the feasibility of a detailed 3-night sleep assessment protocol in a small cohort of ME/CFS patients • Pilot of the most comprehensive sleep study ever attempted in ME/CFS • Mixed methods; • functional assessments • actigraphy • sleep diary • ambulatory PSG • sampling of diurnal salivary cortisol • Naturalistic setting • 3-nights
Study flow 12-month study period Flow Diagram of Study (recruitment, protocol and analytical) Process OSA, obstructive sleep apnea; PSG, polysomnography; CAR, cortisol awakening response
Study flow 12-month study period Flow Diagram of Study (recruitment, protocol and analytical) Process OSA, obstructive sleep apnea; PSG, polysomnography; CAR, cortisol awakening response
Study flow 12-month study period Flow Diagram of Study (recruitment, protocol and analytical) Process OSA, obstructive sleep apnea; PSG, polysomnography; CAR, cortisol awakening response
Sequence of performing the polysomnograph 4 • EEG, EOG, chin EMG • Thermal flow & pressure sensor (applied shortly before bedtime) • Snore sensor Polysomnography (PSG) is the most important laboratory technique for assessment of sleep and its disorders. PSG records multiple physiological characteristics simultaneously during sleep. Applying the electrodes and sensors is the most important part of the sleep study to ensure quality data. 1 2 4 • ECG • Thoracic & abdominal belts • Position sensor 3 • Pulse Oximeter (appled shortly before bedtime) • Actiwatch (additional to PSG) 4 • Leg EMG Reassure the patient and explain what each sensor measures
Raw (PSG) Data REM Fig. 1.: PSG data - EEG signals (electrodes T3, T4, FPZ, FP1, FP2, F3, F4, CZ, C3, C4, P3, P4, O1, O2), EOG & EMG signals, ECG and the respiration signals.
Preliminary sleep data Main Outcome Measures of interest (nights 2 & 3 only): • Total Sleep Time • Sleep Onset Latency • Awakenings – number & duration • Sleep Efficiency (%) • % of each stage & wake (of TSP) • REM Latency • Stage transitions Sleep Continuity Sleep Architecture TSP, total sleep period; NREM, non rapid eye movement; REM, rapid eye movement
Preliminary sleep data Comparison of Patients & Controls Independent samples t–test for the objectively-derived sleep variables (mean night 2 & night 3), between patients (CFS) and control participants. Awakenings a key feature! Controls lab-based but ok not looking at N1 eliminate first-night effect *p ˂ .05, ** p ˂ .01, *** p ˂ .001. SOL, sleep onset latency; WASO, wake after sleep onset; TST, total sleep time; N1, stage 1 sleep; N2, stage 2 sleep; SWS, slow wave sleep; REM, rapid eye movement sleep; SEI, sleep efficiency index; TSP, total sleep period; NWAK, number of awakenings
Main outcomes 4 • Was the sleep assessment feasible? • YES! Successful protocol: methods acceptable to patients • No drop-outs, highly motivated • Tolerated procedures (minor considerations) • Adherence to sleep & cortisol protocol / Fidelity to timing 4 • Preliminary sleep data: • Increased amounts of light sleep & wakefulness • Established temporal stability of sleep variables over 2 nights • Cortisol data currently being analysed • Possible to develop future trial with this protocol
Conclusions & Implications Research Clinic • Established a feasible (comprehensive) protocol to assess sleep & cortisol in ME/CFS • 1 night affords detection of PSD • 2 nights sufficient to capture sleep physiology of patients • Consider daytime sleep (24h PSG assessment ) • ‘Light sleep’ a feature throughout – follow up potential issues with cortical arousal? • Consider sleep in the context of other factors (i.e. adjustment to illness, severity of illness, differential management) • Need to routinely screen for PSDs in patients presenting with ME/CFS – early on! • Different groups (sleep phenotypes) with different sleep profiles that may be treated for their sleep in different ways • Clinicians should be mindful of these sleep- phenotypes when tailoring sleep-based interventions for ME/CFS patients • Target disturbed sleep & napping during treatment may improve other symptoms (i.e. fatigue , cog functioning)
Current Work …Applying the research in a clinical setting Development of a sleep intervention for people with ME/CFS CRESTA Fatigue Clinic (Clinics for Research and Service in Themed Assessment) Supported by the ME Association
Acknowledgements Prof Julia Newton Dr Vincent Deary Prof Jason Ellis Dr Mark Wetherell Dr Pierre de Roy and his team, VermoeidheidCentrum, Lelystad Study Participants Funding: Action for ME, ME Association Northumbria Centre for Sleep Research
Stay Connected… zoe.gotts@northumbria.ac.uk Contact.. Northumbria Centre for Sleep Research ME / CFS Research Newcastle Find us.. @NCSR_Sleep @MECFSResNew Follow us..