Download
1 / 28
290 likes | 549 Views
Mononuclear Leukocytes and Chronic Inflammation Wednesday, September 25, 2002. Reading- Chpt. 4. Definition of Chronic Inflammation.

E N D
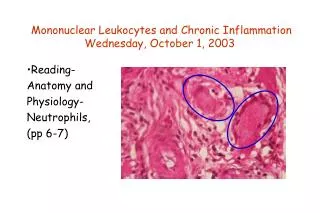
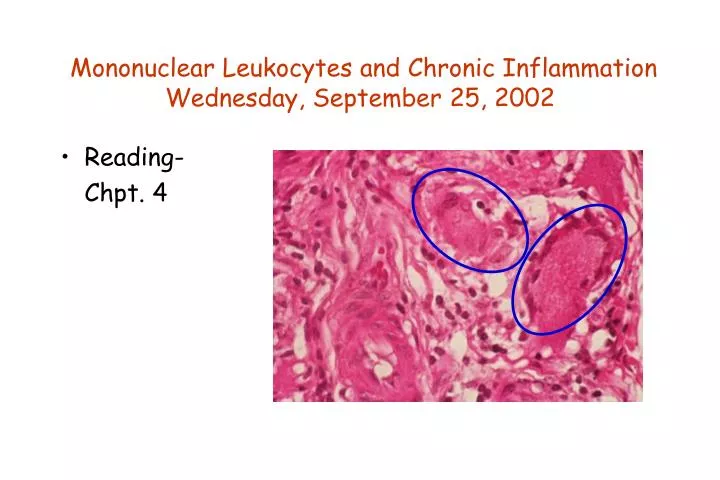
Mononuclear Leukocytes and Chronic InflammationWednesday, September 25, 2002 • Reading- Chpt. 4
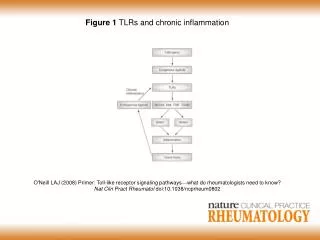
Definition of Chronic Inflammation •Chronic inflammation is an inflammatory response of prolongedduration, which is provoked by persistence of the causative stimulus to inflammation in the tissue. •The inflammatory process inevitably causes tissue damage and is accompanied by simultaneous attempts at healing and repair. •The exact nature, extent and time course is variable, and depends on a balance between the causative agent and the attempts of the body to remove it.
Cells and Mediators •Histological hallmarks of chronic inflammation are: 1) infiltration by mononuclear cells, principally monocytes/ macrophages and lymphocytes; 2) proliferation of fibroblasts, and in many instances, small blood vessels (endothelial cells); 3) increased connective tissue (fibrosis); and 4) tissue destruction.
General Functions of Phagocytic Cells •Clearly defined role as a scavenger of senescent/damaged cells. •And, as a powerful defense mechanism against m'organisms. •Biochemical activities that are cytolytic or destructive. •Have the capacity to damage host tissue. •When destruction occurs, either as a by-product of cell combat or duringhost autoimmune disorders, phagocytes contribute to inflammation and host cell destruction. •Target range of phagocytes is relatively non-specific, and they depend on the lymphoid system for directions.
Monocytes •Largest cell in the bloodstream. •Monocytes are the most closely related cell to neutrophils, but they have numerous differences. •Monocytes are less numerous in the bloodstream than neutrophils, but they play an important role in the activation and function of the immune system. •Neutrophils are termed end-stage cells, that is, the final form of differentiation.
Monocytes (cont’d) •Monocytes are considered intermediate-stage cells, and they can further develop to macrophages. •Other differences include the shape of the nucleus- segmented in neutrophils and singular in monocytes. •Neutrophils have numerous granules that are quite visible, monocytes do not have as many and they are much less visible.
Functions of Monocytes •Defense against pathogenic organism invasion-- "phagocytosis" •Activation of acquired immune response •Defense against host cells infected by pathogens/cancer •Scavengers •Produce "monokines" (that is, cytokines) and growth factors
Example of Chronic Inflammation Two pulmonary granulomas, which typically consists of epithelioid macrophages, giant cells, lymphocytes, and fibroblasts.
Regulation of Monocyte Production •Proliferation and maturation in bone marrow takes 5-6 days, similar to neutrophils and other granulocytes. •Monocytes remain in the circulation for 2-3 days. •Once they leave the blood stream, they do not return. •Intissues, they undergo blast formation and become immature macrophages, after a number of cell divisions they are mature macrophage ("histiocyte"). •Mature macrophages may live for months to years!
Leukocyte Recognition of Pathogens •Fc receptor (FcR) for antibodies (adaptive immunity): --Specificity --Phagocytosis --Specialized functions •Fc receptors recognize antigens via antibodies. •Fc receptors transduce signals. •Fc receptors activate or inactivate leukocytes.
•FcR bind to specific classes of Ig: -FcgR to IgG -FcµR to IgM -FceR to IgE •Phagocytes express FcgR -3 subtypes FcgRI, RII, RIII •Antibodies bind to multivalent pathogen •FcR bind to Fc portion of cluster of antibodies •FcR aggregate •Intracellular signals Features of Fc Receptors
Activating Fc Receptor Function • •FcgRI activation trigger macrophage • -ROS, cytokines, phagocytosis • •FcgRIIA activation trigger neutrophil • -ROS • •FceRI triggers basophils and mast cells • -Degranulation • •FcgRIIIA triggers natural killer cell • -Degranulation (perforin + granzyme B)
Chronic Inflammation •Overall concept of inflammation is relatively straightforward: --host-defense response to invading substance; --excluding autoimmune events, inflammation occurs due to some kind of insult or injury; --if the cause is not removed, acute inflammation becomes chronic and can persist for months, years, a lifetime!
Chronic Inflammation (cont’d) •Inflammatory process goes from the "fire" of the cardinal signs of inflammation (acute)to now become a "simmer" (chronic): --that is, the two signs that relate to "flames", redness and heat, are toned down but swellingandpain remain.
Chronic vs. Acute Inflammation--A Few "Differences" •Microscope will tell you what going on when inflamed tissue is examined: --it can tell us why the inflammatory response is not turned off by showing us that the offending agent is still there. --in acute inflammation the hallmark cell is the neutrophil, while in chronic inflammation, mononuclear leukocytes are predominant.
Chronic vs. Acute Inflammation--A Few "Differences“ (cont’d) •Initial event of inflammation is the local recruitment of blood components: --the acute response takes place almost immediately, seconds or minutes after the injury: --fluids pour out and then the neutrophils. --the chronic response then takes over if the injurious agent is not immediately removed. Its function is a more sophisticated defense than phagocytosisalone.
Acute Inflammation vs. Chronic Inflammation Inflammation may have one of four outcomes: 1. complete resolution- restoration of the site of acute inflammation to normal: --outcome when the injury is mild (superficial cut, burn or trauma, little tissue injury); 2. healing by scarring-substantial tissue destruction, or when inflammation occurs innon-regeneratingtissues; 3. abscess formation- occurs in infections with pyogenic organisms; 4. progresses to chronic inflammation.
Causes of Chronic Inflammation Clinically, chronic inflammation arises in various organs: 1. It may follow acute inflammation-persistence of the inciting stimulus, or interference in the normal process of wound healing. --example, lung infections that persists and leads to tissue destruction, and a chronic lung abscess. 2. Repeated bouts of acute inflammation- the patient shows successive attacks of fever, pain, and swelling. --occurs in recurrent infections in major organs.
Causes of Chronic Inflammation (cont’d) 3.More curiously, chronic inflammation may begin insidiously- a low-grade smoldering response that does not follow classic symptoms of acute inflammation. --This includes some very disabling human diseases: •rheumatoid arthritis •tuberculosis •and chronic lung disease
Causes of Chronic Inflammation (cont’d) •These diseases mentioned above occur in the following setting: a. persistent infection by intracellular microorganisms --tubercle bacilli, viral and fungal infections, which are of low toxicity but evoke an immunological reaction;
Causes of Chronic Inflammation (cont’d) • b. prolonged exposure to non-degradable but potentially toxic substances (e.g., silicosis and asbestosis); c. immune reactions, particularly those perpetuated against the individual's own tissues (autoimmune diseases, such as rheumatoid arthritis).
Types of Chronic Inflammatory Cells 1. Lymphocytes and macrophages: This illustration shows a mixed chronic inflammatory cell infiltrate containing mainly lymphocytes and macrophages.
Types of Chronic Inflammatory Cells (cont’d) • Lymphocytes around a blood vessel: • Perivascular cuffing is a common pattern of lymphocytic infiltration in chronic inflammatory reactions. This example is from an inflammatory disease of the brain- multiple sclerosis.
Types of Chronic Inflammatory Cells (cont’d) 3. Macrophages in infarcted brain: Macrophages are very phagocytic, and engulf and degrade all sorts of debris in damaged areas. The macrophage cell bodies are large and round, distended with pale, foamy looking lipid-filled vacuoles.
Types of Chronic Inflammatory Cells (cont’d) • Plasma cells: • These distinctive looking cells have an eccentrically placed nucleus with coarse, blotchy staining of the chromatin, said to resemble a clock face. Plasma cells are mature, end-stage cells of the B-lymphocyte lineage, specialized for antibody production and secretion.
Types of Chronic Inflammatory Cells (cont’d) • Lymphoid follicles: • A lymphoid follicle producing lymphocytes in thyroid tissue during the chronic inflammatory process, Hashimoto's Disease. Inflammation is triggered against its own thyroid tissue, i.e., an autoimmune disease; the packed mature lymphocytes are recognizable by their small, intensely blue/black nuclei.