Download
1 / 59
590 likes | 806 Views
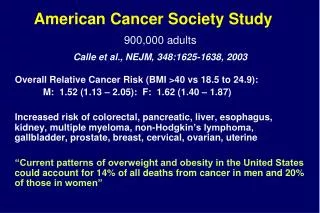
*p<0.05 compared to no ZDV prophylaxis Wade et al, NEJM, 339:20, 11/12/98; 1409-1414. NYS Survey of Childbearing Women HIV Prevalence by Year of Delivery: 1988 - 2001.

E N D
*p<0.05 compared to no ZDV prophylaxis Wade et al, NEJM, 339:20, 11/12/98; 1409-1414.
NYS Survey of Childbearing WomenHIV Prevalence by Year of Delivery: 1988 - 2001 Since 1990, there has been a 60% decline in the number of HIV-infected women giving birth in NYS (1,898 in 1990 to 758 in 2001) Source: New York State Perinatal HIV Surveillance Program
Trends Among HIV-Infected Pregnant Women Source: New York State Perinatal HIV Surveillance Program
Lessons Learned So Far • In the Prenatal Setting: • Mainstreaming HIV C&T into prenatal care is key! • It is important for the MD to reinforce the benefits of early prenatal HIV testing. • Approach the patient early (first prenatal visit) so that blood specimen can be drawn with other prenatal tests. • Later in pregnancy, assess the need to retest (based on risk).
Lessons Learned So Far • In the Obstetrical Setting: • Encourage feeder clinics/private practitioners to transfer prenatal records to labor and delivery (L&D) at a designated point in time (e.g., at 28 weeks) • Encourage the use of a summary sheet with a prominent location for documentation of prenatal HIV status (documentation must include the date of prenatal testing along with a test result). • Conduct HIV test history assessment when the woman presents in L&D
Lessons Learned So Far • In the Obstetrical Setting (cont’d): • Counsel and encourage expedited testing for those with no HIV test documentation (the message is important!) • Remember the goal of early ART – to begin during the intrapartum period if at all possible • Keep a log of expedited tests done. Note: are the patients primarily walk-ins, or are they in the care of a particular clinic or private practitioner?
Lessons Learned So Far • Strategies to Overcome Barriers • Conduct needs assessment to identify barriers unique to your facility. • Focus on issues of concern. • Use continuing quality improvement strategies to address barriers identified (inservice seminars, grand rounds, record keeping). • Still have questions? Call Regulatory Unit Staff – Sheila Hackel or Ellen Kowalski at 518-486-6048.
Rapid HIV Testing - Option 1 A laboratory that does not already hold a permit in the HIV testing category must apply to CLEP to add the testing category and: • Validate the method,train users; • Develop QA protocols and follow NYS Laboratory Standards for QC; • Participate in an expedited proficiency testing and on-site survey process.
Rapid HIV Testing - Option 2 Now that there is a rapid HIV test (OraQuick) available as a CLIA-waived product, birth facilities can apply to CLEP to register the labor and delivery suite or other area as a Limited Testing Site, and perform the test independently of the main laboratory.
Rapid HIV Testing - Option 2 Facilities that choose to perform the OraQuick test under a Limited Testing Site Registration must apply to CLEP and: • Train users, develop QA protocols, and follow the manufacturer’s requirement for QC; • No proficiency test or on-site survey is required.
Rapid testing in Labor and Delivery Stephen Nicholas, M.D. Associate Professor of Clinical Pediatrics College of Physicians and Surgeons, Columbia University, New York City Director of Pediatrics, Harlem Hospital Center
Rapid testing in Labor and Delivery • Since 1999, New York State has had mandatory “expedited testing” • Currently, results of the expedited HIV screening test must be available within 48 hours after the specimen is collected
At present the median time at which HIV-exposed babies found by rapid testing start ARV prophylaxis is 22.5 hours of life Rapid testing in Labor and Delivery
Rapid testing in Labor and Delivery • Most “expedited testing” sites are not open 24 hours a day--the tests are often batched and have been delayed for as long as 127 hours after birth
Interventions • Antiretroviral prophylaxis before birth (ZDV or Nevirapine) • Schedule Cesarean Section (if the mother is not yet in labor) • Decisions about breast or bottle feeding
FDA-approved November 7, 2002 for use with fingerstick whole blood specimens
Reactive Control Positive HIV-1/2 Positive Negative Read results
OraQuick Test Performance Source: OraSure Technologies, OraQuick Package Insert 4/03
Perinatal Screening: The CDC-Sponsored “MIRIAD Study” • Testing of pregnant women in labor for whom no HIV test results are available; • 12 hospitals in 5 cities: Atlanta, Chicago, Miami, New Orleans, New York
Perinatal Screening: MIRIAD Study • 1771 women screened • 12 new HIV infections identified • No false positives, no false negatives