Download
1 / 52
550 likes | 856 Views
Introduction to At-Risk Mental States . Why are we doing this work?. Introduction. What is the rationale behind detecting psychosis early – is there a need? What do ‘at-risk’ clients look like Thinking about Services A very brief history…. Psychosis: The Early Course.

E N D
Introduction to At-Risk Mental States Why are we doing this work?
Introduction • What is the rationale behind detecting psychosis early – is there a need? • What do ‘at-risk’ clients look like • Thinking about Services • A very brief history…
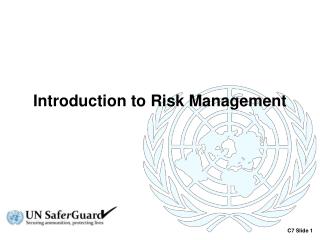
Psychosis: The Early Course Adapted from Larsen et al., 2001 Psychosis premorbid phase very early symptoms psychotic symptoms Treatment & Recovery Relapse? The typical course of psychosis
Psychosis: The Early Course Adapted from Larsen et al., 2001 Psychosis “DUP” premorbid phase very early symptoms psychotic symptoms Treatment & Recovery Relapse? The typical course of psychosis
Psychosis: The Early Course Adapted from Larsen et al., 2001 Early Intervention after onset of psychosis (EIS) Psychosis “DUP” Tertiary Prevention premorbid phase very early symptoms psychotic symptoms Treatment & Recovery Relapse? The typical course of psychosis
Psychosis: The Early Course Adapted from Larsen et al., 2001 Early Detection & Intervention in the at-risk phase (ED:IT) Early Intervention after onset of psychosis (EIS) Psychosis “DUP” Tertiary Prevention premorbid phase very early symptoms psychotic symptoms Treatment & Recovery Relapse? The typical course of psychosis
Is there a need..? ‘Every year across the UK about 7,500 people will develop a first episode of psychosis, onset usually occurring in young people… …this can lead to long term problems, sometimes life long, which leave people on the margins of society, struggling to maintain relationships, or get a job, an income or a home. As many as one in ten die by suicide, often within the first five years, and their families, friends and communities often carry huge burdens of care.’ (report on early detection & intervention - Parker et al 2007)
Is There a Need? • Duration of Untreated Psychosis (DUP) remains approx. one year after onset of psychosis • Poorer outcome related to length of untreated psychosis (Drake et al. 2000; Yung et al. 2003) • Significant disability associated with prodrome (Yung et al., 1996) • Between 5 -15% of individuals with Schizophrenia will commit suicide – most within the first six years of psychosis (Melle et al. 2006) • Often the individual and family are in distress
Other Positives to earlier detection • Intervening early may improve engagement with services (when insight is intact) • Reduce the trauma of hospitalisation & use of M.H. act • Intervening early may reduce psycho-social deterioration
Other Positives to earlier detection • Intervening early may improve engagement with services (when insight is intact) • Reduce the trauma of hospitalisation & use of M.H. act • Intervening early may reduce psycho-social deterioration • The possibility to PREVENT psychosis in vulnerable young people??
What do at-risk clients look like? Employ PACE ‘at-risk’ criteria to identify: • Familial risk plus reduced level of functioning in past yr • or Attenuated psychotic symptoms • or Brief, Limited, Intermittent Psychotic Symptoms • Aged 16-35 years Plus: Evidence of distress & difficulty
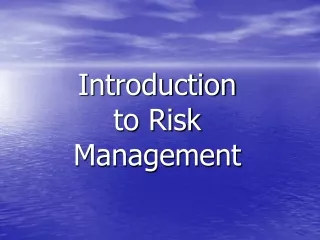
EPOS European Prediction of Psychosis Study Cologne Berlin Amsterdam Turku Birmingham Manchester EPOS : an international prospective study of transition to psychosis in individuals at ‘ultra high risk’
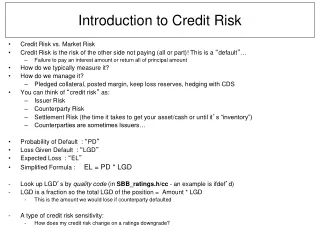
Participants with Suicidal Ideation at Baseline (BDI) - 55% n=232 I would like to kill myself if I had the chance I would like to kill myself I've thoughts of killing myself, but I won't carry them out I don't have any thoughts of killing myself 0.0% 10.0% 20.0% 30.0% 40.0% 50.0% Percent
Cannabis use of high risk patients EPOS Study sites (n: 246)
Transition rate high risk patients EPOS study centres (n=246)
Treatment methods measured in EPOS included: - Medication (sorted by type e.g. Antipsychotic; Anxiolytic; Antidepressant.. - Psychological Therapy (sorted by type e.g. CBT; Psychotherapy.. - Monitoring (telephone / face to face etc) - Group Therapies (e.g. for Social Anxiety) - Family Interventions (e.g. Psychoeducation)
Medication and Psychological Therapy D Fin NL UK Mean Any psychotherapy (%) 41 62 36 95 59 Any meds(%) 36 75 32 50 43 Neither(%)41 16 57 - 28
Medication and Psychological Therapy D Fin NL UK Mean Any psychotherapy (%) 41 62 36 95 59 Any meds(%) 36 75 32 50 43 Neither(%)41 16 57 - 28SIPS+8.7 9.1 11.6 10.2 9.7
Medication and Psychological Therapy D Fin NL UK Mean Any psychotherapy (%) 41 62 36 95 59 Any meds(%) 36 75 32 50 43 Neither(%)41 16 57 - 28SIPS+8.7 9.1 11.6 10.2 9.7 Transition rate (%)7.7 10.9 29.8 11.9 14
Medication and Psychological Therapy D Fin NL UK Mean Any psychotherapy (%) 41 62 36 95 59 Any meds(%) 36 75 32 50 43 Neither(%)41 16 57 - 28SIPS+8.7 9.1 11.6 10.2 9.7 Transition rate (%)7.7 10.9 29.8 11.9 14 Expected Transition without Intervention:35 – 54% (SIPS/CAARMS)
Treating ‘at-risk’ clients • Confusion as to how to treat this cohort – not ‘psychotic’ but very unwell… • Little evidence as to the relative effectiveness of medication / psychological therapies / case management • Guidelines for treatments for HR group developed by International Early Psychosis Association (2005) but not consistently adopted by local services • Early Detection Report (Parker et al 2007) – suggested guidelines
Developing a Service Approach Early Detection Education, Awareness-raising, Training Engagement, Appropriate client/family Treatments Accurate- assessment, Evaluation
Developing a Service Approach Early Detection Education, Awareness-raising, Training
Stigma – Public Attitudes to Mental Illness • 83% agreed society needs to adopt a more tolerant attitude • 89% agreeing that society has a responsibility to provide people with the best possible care • 74% agreed that mental illness is an illness like any other • 20% said there is something about people with mental illness that makes it easy to tell them from normal people Department of Health Survey (2003) : http://www.doh.gov.uk/public/england.htm (1897 adults, 16+)
Stigma – Public Attitudes to Mental Illness 2 • 25% agreed that people with mental illness should be excluded from public office and 16% said they should never be given any responsibility • Only 21% of respondents agreed that women who were once in hospital for mental illness can be trusted as a babysitter (31% neither agree/disagree) • 62% agreed that they would not want to live next door to someone who has been mentally ill • 60% agreed that a woman would be foolish to marry a man who has suffered from mental illness, even if he seems fully recovered Department of Health Survey (2003) : http://www.doh.gov.uk/public/england.htm (1897 adults, 16+)
Stigma & Psychosis • 70% of respondents rated people with schizophrenia as dangerous to others • 80% rated people with schizophrenia as unpredictable • 60% rated people with schizophrenia as difficult to talk to • 50% thought people with schizophrenia would never recover Crisp, A.H., et al. (2002). British Journal of Psychiatry, 177, 4-7. (1737 adults 16+)
TIPS – Norway DUP can be dramatically reduced through educational campaigns
ED:ITMental Health Promotion • ‘Mental health & Psychosis’ workshops for individuals working with young people (300 + attended) • ‘Lunchtime workshops’ for MH professional staff - training in ‘Early Identification’ of psychosis (200 + attended) • Educational DVD’s created by service users of the Early Intervention Services • ‘REDIRECT’ educational project for GP’s in ‘Early Signs’ of psychosis – reducing DUP
Developing a Service Approach Early Detection Engagement, Appropriate client/family Treatments
Which Therapy for at-risk clients? • Evidence base for effectiveness of different treatments for HR clients remains sparse • Psychological therapy suggested as more acceptable, less stigmatising to HR clients(Bentall & Morrison 2002) • Possible risk of pharmacological side-effects and high non-adherence if antipsychotics used (eg McGlashan et al. 2006) • Co-morbid symptoms (anxiety/depression etc) addressed by psychological interventions
Interventions – Birmingham ED:IT flexible treatment options including … ED:IT Sept 2004
EDIE2 (MRC funded UK Intervention Trial 2006 - 2010) • MRC funded Trial of CBT for individuals at high risk of psychosis • Aim to recruit n=320 high-risk participants • To reduce transition to psychosis and reduce the distress felt by help-seeking individuals • Inclusion using PACE at-risk criteria
What sites are involved in EDIE 2? • Manchester (lead site) • Glasgow • Birmingham/ Worcester • East Anglia • Cambridge Check EDIE2 website at University of Manchester
That’s the theory… but does it work in practice? • Are we able to ‘detect’ young people in the pre-psychotic phase in the community? • Do these young people actually want help from (mental health) services? • Is the ‘help’ that we are offering acceptable to young people?
That’s the theory… but how is it working in practice? • Are we able to ‘detect’ young people in the pre-psychotic phase in the community? • Do these young people actually want help from (mental health) services? • Is the ‘help’ that we are offering acceptable to young people? YES
A very Brief History of treatments for Psychosis (to remind us where we’ve been…)
Dunking Pool 1403 - St Mary of Bethleham hospital near London first accepts psychiatric patients (from 1776 this was also a tourist attraction)
1890 - Dr Gottlieb Burkhardt attempts to alter behaviour in 6 severely agitated Swiss patients by extracting portions of their frontal lobes (2 died) Lobotomy Kit (NHS outreach model)
Portable ECT Machine 1913 - Emil Kraepelin categorises mental illnesses into those which could be cured and those which could not (e.g.dementia praecox - psychosis) 1938 - Cerletti and Bini introduce electroshock convulsions
1952- Deniker Leborit & Delay discover the antipsychotic properties of chlorpromazine marking the beginning of psychopharmacology 1955- More than 55,000 men women and children in the US undergo lobotomy
1985 - Ian Falloon trains GP’s to identify ‘early signs’ of psychosis 1990’s- EPPIC / PACE establish Early Detection/Intervention Clinical & Research programmes in Melbourne - Early Intervention approaches introduced in UK and Internationally - TIPS Norweigian educational campaigns reduce DUP 2000’s– First Early Detection / Prevention Programmes in UK EDIE(2), ED:IT, OASIS, REDIRECT, BRITE
1985 - Ian Falloon trains GP’s to identify ‘early signs’ of psychosis 1990’s- EPPIC / PACE establish Early Detection/Intervention Clinical & Research programmes in Melbourne - Early Intervention approaches introduced in UK and Internationally - TIPS Norweigian educational campaigns reduce DUP 2000’s– First Early Detection / Prevention Programmes in UK EDIE(2), ED:IT, OASIS, REDIRECT, BRITE That’s a big jump in 20 years…