Download
1 / 1
10 likes | 217 Views
Anatomical Considerations for Urolithiasis in the Morbidly Obese. Jonathan Witten MD, Jason Smith MD, Brian Duty MD, Michael Conlin MD Department of Urology, Oregon Health & Science University. Results. Introduction.

E N D
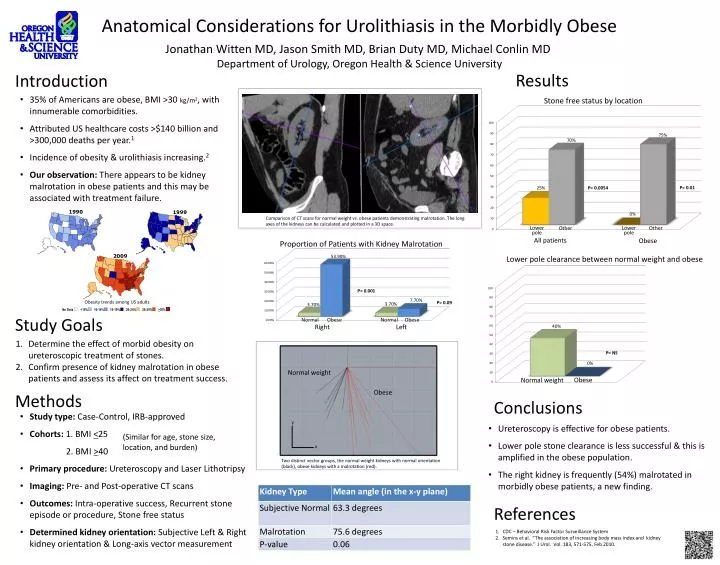
Anatomical Considerations for Urolithiasis in the Morbidly Obese Jonathan Witten MD, Jason Smith MD, Brian Duty MD, Michael Conlin MD Department of Urology, Oregon Health & Science University Results Introduction • 35% of Americans are obese, BMI >30 kg/m2, with innumerable comorbidities. • Attributed US healthcare costs >$140 billion and >300,000 deaths per year.1 • Incidence of obesity & urolithiasis increasing.2 • Our observation: There appears to be kidney malrotation in obese patients and this may be associated with treatment failure. Stone free status by location P= 0.01 P= 0.0054 1990 1999 Comparison of CT scans for normal weight vs. obese patients demonstrating malrotation. The long axes of the kidneys can be calculated and plotted in a 3D space. 1990 1999 Other Other Lower pole Lower pole All patients Obese Proportion of Patients with Kidney Malrotation 2009 Lower pole clearance between normal weight and obese P= 0.001 Obesity trends among US adults P= 0.09 25-29% 15-19% 20-24% No Data <10% 10-14% >30% Study Goals Obese Normal Obese Normal Right Left Determine the effect of morbid obesity on ureteroscopictreatment of stones. Confirm presence of kidney malrotationin obese patients and assess its affect on treatment success. P= NS Normal weight Obese Methods Obese Normal weight Conclusions • Study type: Case-Control, IRB-approved • Cohorts: 1. BMI <25 • 2. BMI >40 • Primary procedure: Ureteroscopy and Laser Lithotripsy • Imaging: Pre- and Post-operative CT scans • Outcomes: Intra-operative success, Recurrent stone episode or procedure, Stone free status • Determined kidney orientation: Subjective Left & Right kidney orientation & Long-axis vector measurement y • Ureteroscopy is effective for obese patients. • Lower pole stone clearance is less successful & this is amplified in the obese population. • The right kidney is frequently (54%) malrotated in morbidly obese patients, a new finding. (Similar for age, stone size, location, and burden) x Two distinct vector groups, the normal weight kidneys with normal orientation (black), obese kidneys with a malrotation (red). References CDC – Behavioral Risk Factor Surveillance System Seminset al. “The association of increasing body mass index and kidney stone disease.” J Urol. Vol. 183, 571-575, Feb 2010.