Download
1 / 27
280 likes | 497 Views
Incontinentia Pigmenti: Case report and Literature review. 高雄榮民總醫院皮膚科 黃郁菁 陳雅惠 羅珮瑜 宗天一. Basic information. Age: 4 day-old Gender: female Birth history: Mother age: 33 year-old G2P1A1, GA: 38+ weeks, BBM: 3440 gm, via C/S without perinatal insult. Chief complaint:.

E N D
Incontinentia Pigmenti: Case report and Literature review 高雄榮民總醫院皮膚科 黃郁菁 陳雅惠 羅珮瑜 宗天一
Basic information • Age: 4 day-old • Gender: female • Birth history: Mother age: 33 year-old G2P1A1, GA: 38+ weeks, BBM: 3440 gm, via C/S without perinatal insult
Chief complaint: • Numerous small red infiltrative papules and confluent into plaques since birth • The papaules and plaques became vesicles 4 days after birth; spread over trunk, perineal area, four limbs ; less on abdomen, worse over dependent site
Present illness • No fever, No oral ulcer Darier’s sign: negative, • Lab data:
Differential diagnosis • Incontinential pigmenti • Epidermolysis bullosa • Erythema toxicum neonatorum • Viral exanthem ( HSV IgM: negative)
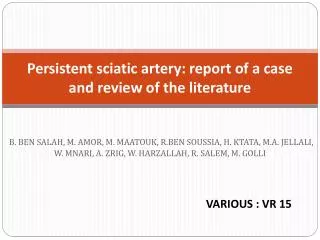
Progress 2 weeks later 4 weeks later
2 weeks later Progress 4 weeks later
6 months later Progress
Family history Hypopigmentation over axillae; alopecia; dental carriers
Ophthalmology finding • 1 month-old → Retinal hemorrhage with VH, OD • 3 month-old →Retinal detachment, OD post pan- retinal laser photocoagulation
Diagnosis and Treatment • Incontinentia pigmenti • Treatment : #Skin: applied with topical steroid; # Consult ophthalmologist immediately after diagnosis #Be ware of neurology symptoms and dentition
Discussion • Occuring in 1 in 50000 newborns • X-linked dominant systemic disorder • IP1 and IP2 Cutis, May 2007; Vol. 79, P.355
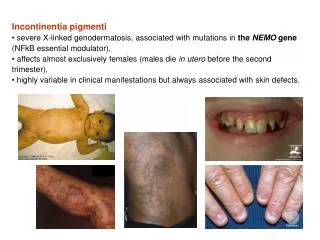
*Only females (37:1) * Rare males( XXY, somatic mosaicism, hypomorphic allele) Pathophysiology Mutation of gene for NEMO (Located on Xq28) ↓ Inactivate the transcription factor nuclear factor KB (NF-kb) ↓ Cells lack of protection from apoptosis in response to TNF-alpha ↓ Teeth Eye Skin, hair, nail Neurologic defect
Nature Vol 405 25 May 2000 J Am ACAD Dermtaol August, 2002; 47: 169-87
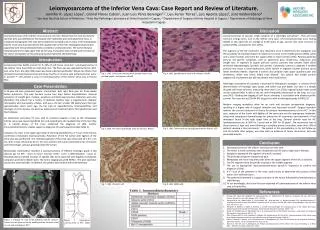
Clinical presentation-Skin (Stage I) • At birth or shortly thereafter; 90% • Liner arrangements of erythema, vesicles, and pustules, and occasionally bullae follow lines of Blaschko • Usually clear by 4-month old; may reactive following infectious event Spongiotic dermatitis with numerous eosinophils, vacuolated basal cells
Clinical presentation-Skin (Stage II) Papillated epidermal hyperplasia, with dyskeratotic cells, hyperkeratosis, acanthosis 1.beginning approximately 2-6 weeks; resolve before 6 month; 70 % 2.Linear verrucous cluster of papulonodules
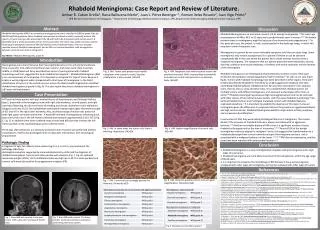
Clinical presentation-Skin (Stage III) 1.Beginning approximately at age 12 to 40 weeks ; resolve in puberty ; 98 % 2.Macular hyperpigmentation in a swirled pattern along the lines of Blaschko 3.Often involve nipples, axillae, groin Thickened papillary dermis; many melanophage, deposit of melanin in dermis
Clinical presentation • Stage IV →Hypopigmentation; 42 % →Present from early teens through adulthood • Hair: Diffuse scarring alopecia; often on the vertex • Nail: Onychodystrophy can involve all of the fingernails and toenails • Teeth: Delayed dentition; anodontia; hypodontia; misplaced and deformed teeth • Occular manisfestations: Strabismus; retinal detachment; peripheral retinal avascularity; preretinal fibrovascular proliferation with vitreous hemorrhage Cutis, May 2007; Vol. 79, P.355
Clinical presentation • Neurologic manifestation: occurring in approximately 1/3 of cases Seizures may be the dominant features • Immunologic derangements: related to cutaneous and pulmonary TB associated with male cases of IP and the related syndromes of ectodermal dysplasia and immunodeficiency (EDA-ID) • Other manifestations: cardiovascular: ex: pulmonary hypertension Muscular system: ex: short limbs Cutis, May 2007; Vol. 79, P.355
Advances in genetic and pathophysiology • NEMO (nuclear factor κB essential modulator) or IKKγ (γ-subunit of the inhibitor κB kinase) IκB (inhibitor κB ) IKK (inhibitor κB kinase) IKK : IKK α, IKKβ (catalytic) IKK γ (modulator) NF- κB (Nuclear factor κB ) Regular inflammation, confer antiapoptotic reaction
Treatment • Skin: do not require specific treatment, spontaneous resolution *Vesicular stage is best managed with sterile dressings to prevent bacterial superinfection *Use of lasers in the treatment of hyperpigmentation should be discouraged (Australas Dermatol 1997; 38:155-7) • Nail: subungual and periungual tumors must be managed promptly (surgical excision, following bony curettage) • Consult Ophthalmologist immediately after diagnosis • Consult Neurologist if neurologic symptoms present