Download
1 / 26
260 likes | 383 Views
Ductal Carcinoma in situ. David M. Euhus, MD, FACS Professor of Surgery Director, Clinical Cancer Genetics UT Southwestern Medical Center at Dallas. Ductal and Lobular Anatomy of the Breast. Estrogen Receptor Positive Luminal Cell. Estrogen Receptor Negative Luminal Cell.

E N D
Ductal Carcinoma in situ David M. Euhus, MD, FACS Professor of Surgery Director, Clinical Cancer Genetics UT Southwestern Medical Center at Dallas
Estrogen Receptor Positive Luminal Cell Estrogen Receptor Negative Luminal Cell Myoepithelial Cell Stem/Progenitor Cell
Estrogen Receptor Positive Luminal Cell Estrogen Receptor Negative Luminal Cell Myoepithelial Cell Stem/Progenitor Cell
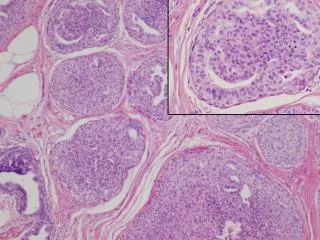
Pathology of Precancerous Changes and DCIS Normal Hyperplasia Atypical Hyperplasia Types of DCIS Cribriform Micropapillary Solid Comedo
DCIS versus Invasive Breast Cancer • Ductal Carcinoma in situ • Means milk duct cancer “in place” • Cancer cells fill the milk ducts but do not “invade” through the wall of the milk duct • Stage 0 breast cancer • Invasive Breast Cancer • Cancer cells invade through the wall of the milk duct • Can get into lymphatic channels and lymph nodes • Can get into blood stream and other organs
Should I have a Breast MRI After I am Diagnosed with DCIS? • About 10% of breast MRIs will prompt additional imaging or a biopsy (3/4 of those biopsies will be benign). • MRI may overestimate the size of the DCIS leading to more extensive surgery. • I only order an MRI if the mammogram or exam make me suspicious that there is more there than meets the eye.
Should I have a Sentinel Lymph Node Biopsy as Part of My DCIS Surgery? • If DCIS was initially diagnosed by core needle biopsy there is a 15% chance that there is actually an invasive breast cancer in the neighborhood. • If all you have is DCIS there is <1% chance that the SLN will be positive. • I don’t do SLN biopsy for pure DCIS if the patient is having a lumpectomy. • I do SLN for DCIS if the patient is having a mastectomy.
What are the Options for Treating DCIS? • Breast Conserving Surgery • Lumpectomy + Radiation • + Tamoxifen (for ER+ DCIS) • Mastectomy
What Happens if I decide Not to Get Treatment for a DCIS? • 28 Small low grade cases treated by biopsy only • 24 year median follow-up Page DL, Cancer 1995;76:1197-200
Up oh. Margins are positive for DCIS Re-excise
If I Have a Lumpectomy for DCIS do I Have to Have 6 ½ Weeks of Radiation Treatments? • Radiation is not as effective against DCIS as it is against invasive cancer. • But radiation can cut the recurrence rate in half. Some women are appropriately treated with 5 days of focused radiation DCIS < 2 cm Age > 50 Not high grade Negative margins Ballon Catheter Radiation CyberKnife
If I Have a Lumpectomy for DCIS can I skip the Radiation Treatments All Together? • Van Nuys Prognostic Index • DCIS size < 1.5 cm • Negative margin > 1 cm • Not high grade • No comedo necrosis • Age > 61 • OncoTypeDx DCIS Recurrence Score
A New Test for Estimating Recurrence Risk After Lumpectomy with No Radiation OncoTypeDX In my mind the recurrence risk is too high even with a low score. I have not used this test. http://www.genomichealth.com/en-US/OncotypeDX.aspx
Double Mastectomy for DCIS • More and more women with DCIS are choosing to have both breasts removed • - About 5% of all DCIS patients • - About 18% of women who need one mastectomy
What is the Risk of Recurrence after DCIS Treatment? • After lumpectomy and radiation there is a 10 – 24% chance that DCIS will recur. • Half of these recurrences are invasive cancer • After mastectomy the risk of recurrences is 2% • The chance of dying of breast cancer after DCIS treatment is <2% • May be a bit higher for African-American women.
Do Some Women with DCIS Have a Higher Recurrence Risk? Factors Associated with Greater Recurrence Risk • Not getting “negative” margins at surgery • Younger age (e.g. <45) • High grade DCIS (very disorganized cells) • Estrogen receptor negative DCIS • Her-2/neu positive DCIS • Larger DCIS
Are there Medications to Prevent DCIS of Reduce the Recurrence Rate? • Tamoxifen (for ER positive) • Reduces DCIS rate by 50% in high risk women • Reduces recurrence after treatment by 40% • Raloxifene • Does not appear to reduce DCIS risk • No recurrence data; not used • Aromatase Inhibitors • Clinical trials being done now • Herceptin (for Her-2/neu positive) • Clinical trials being done now
Summary • DCIS is diagnosed almost exclusively from mammographic screening. • Inadequately treated DCIS can become invasive breast cancer. • Not every DCIS presents a health threat. • We can’t tell which ones are not a threat. • Treating DCIS significantly reduces the risk for invasive breast cancer. • The challenge is not to over treat.
Summary for Young Women • DCIS is very uncommon in young women • Recurrence rates tend to be higher in young women. • A DCIS diagnosis does not impact survival • Lumpectomy + radiation (+ tamoxifen for ER positive DCIS) is a treatment option. • More young women are choosing double mastectomy.