Download
1 / 27
320 likes | 593 Views
Difficult Airway Management Techniques. Facilitated Intubation Algorithm. Developed by Daniel Davis of UCSD Designed to minimize errors during facilitated Intubation. Step #1: Ensuring Ventilation. Difficult airway management requires time.

E N D
Facilitated Intubation Algorithm • Developed by Daniel Davis of UCSD • Designed to minimize errors during facilitated Intubation
Step #1: Ensuring Ventilation • Difficult airway management requires time. • The amount of time you have in the airway is determined by the patient’s oxygenation status, and their general health.
Step #1: Ensuring Ventilation • The most fundamental element of airway management is effective BVM usage. • Using the BVM to it’s full potential requires 4 essential components: • Tight Seal • Jaw Thrust • Sellick Maneuver • NPA/OPA
Step #1: Ensuring Ventilation OPA Sellick’s Tight Seal Head Tilt
Step #2: Predicting Complications • Prior to a facilitated intubation it is important to perform a pre-assessment of your patient for possible complications. • The Mnemonic (FIRST LEMON) will help to guide you in your assessment.
F – Facilitated I – Intubation R – Requires S – Superb T - Techniques L – Look E – External (3-3-2) M – Mallampati O – Obstruction N – Neck (manual ILS) Step #2: Predicting Complications
Step #3: Maximize 1st Attempt • In order to minimize complications, it is important to set yourself up for success on your first attempt to intubate.
Step #3: Maximize 1st Attempt • FlexGuide Stylet • External Laryngeal Manipulation (E.L.M) • Head Elevated Position (H.E.P) • Consider Miller Blade
Step #3: Maximize 1st Attempt E.L.M H.E.P
Step #4: Assemble Team + • Minimum of 2 people, preferably 3 • MUST HAVE • The Intubator • Person to watch the monitor • Optimally a person to assemble equipment
Step #4: Intubator Tasks • Pre-oxygenate (NRB/BVM) • Pre-assessment (First-Lemon) • Determine Equipment needs • Perform Intubation • Verify Placement • Guard Tube Through Call Should be the person with the most experience intubating.
Step #4: Monitor Person Tasks • Ensure Patient is on the heart monitor. • Ensure Pulse Ox is on and functioning. • Have ETCO2 ready. • Input Airway Benchmarks into LP12. (ETT Attempt, ETT Abort, ETT Succ) • Monitor for Desaturation/HR Reactivity and STOP attempt if it occurs. Intubation Task Leader.
Step #4: Equipment Person Tasks • Set up 1st choice blade and Backup. • Set up 1st choice tube, have Backup ready. • Layout FlexGuide, be prepared to remove regular stylet. • Have rescue airway ready. (Combitube) • Have tube tie prepared. • Assist with medication prep/administration. • Serve as intubators right hand. Can be an EMT, proper setup helps to mitigate problems.
1st Attempt Unsuccessful SaO2 in mid-90’s “Can’t Intubate, Can Ventilate” SaO2 < mid-90’s “Can’t Intubate, Can’t Ventilate” • Remember…..Flip a coin. • Provide immediate re-ventilation via BVM. • Next determine SaO2
Anterior Airway • FlexGuide • E.L.M. • H.E.P • Miller Blade
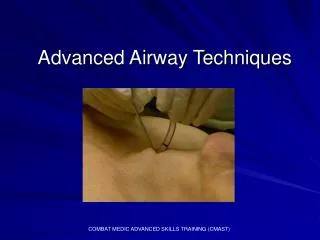
Traumatized/Obstructed Airway • Suction • Magills • Combitube • FlexGuide • Cricothyrotomy
Prevent Hypoxic Arrest SaO2 Above 90% • Consider another intubator, • BVM only • FlexGuide
Prevent Hypoxic Arrest SaO2 Below 90% • Combitube • Cricothyrotomy • BVM
Summary • Facilitated Intubation is a HIGH RISK PROCEDURE • The Goal of all airway procedures is to provide ADEQUATE VENTILATION • By improving the procedure we use to intubate, we can decrease adverse events from occuring.