Download
1 / 8
80 likes | 246 Views
Emergency department point-of-care ultrasound in out-of-hospital and in-ED cardiac arrest Gaspari R, Weekes A, Adhikari S, et al. Resuscitation. 2016;109:33-39. DEEP DIVE SERIES Echo in Cardiac Arrest. Objective - Can POCUS determine outcomes in cardiac arrest? Intervention

E N D
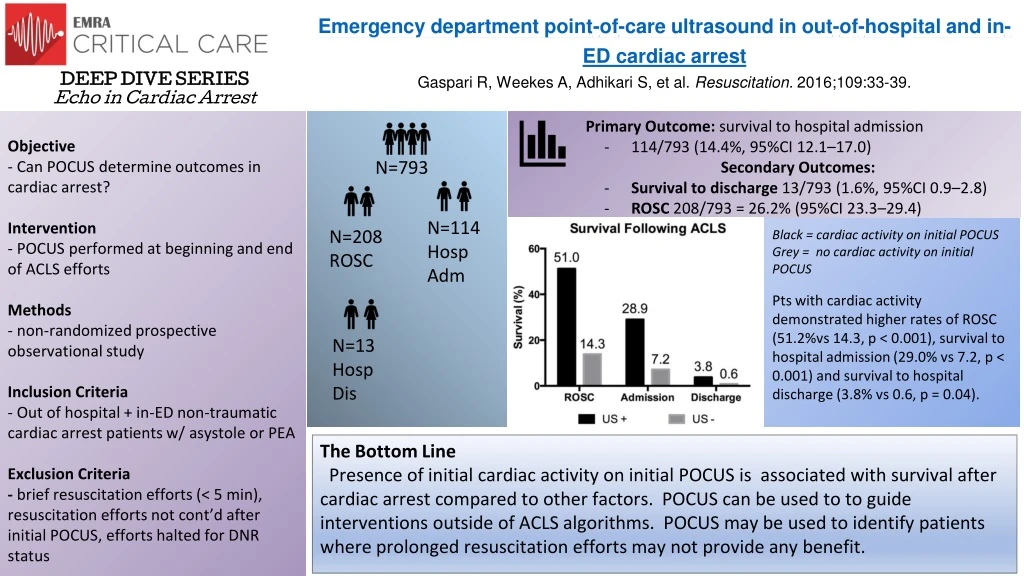
Emergency department point-of-care ultrasound in out-of-hospital and in-ED cardiac arrestGaspari R, Weekes A, Adhikari S, et al. Resuscitation. 2016;109:33-39. DEEP DIVE SERIES Echo in Cardiac Arrest Objective - Can POCUS determine outcomes in cardiac arrest? Intervention - POCUS performed at beginning and end of ACLS efforts Methods - non-randomized prospective observational study Inclusion Criteria - Out of hospital + in-ED non-traumatic cardiac arrest patients w/ asystole or PEA Exclusion Criteria - brief resuscitation efforts (< 5 min), resuscitation efforts not cont’d after initial POCUS, efforts halted for DNR status Primary Outcome: survival to hospital admission • 114/793 (14.4%, 95%CI 12.1–17.0) Secondary Outcomes: • Survival to discharge 13/793 (1.6%, 95%CI 0.9–2.8) • ROSC 208/793 = 26.2% (95%CI 23.3–29.4) N=793 N=114 Hosp Adm Black = cardiac activity on initial POCUS Grey = no cardiac activity on initial POCUS Pts with cardiac activity demonstrated higher rates of ROSC (51.2%vs 14.3, p < 0.001), survival to hospital admission (29.0% vs 7.2, p < 0.001) and survival to hospital discharge (3.8% vs 0.6, p = 0.04). N=208 ROSC N=13 Hosp Dis The Bottom Line Presence of initial cardiac activity on initial POCUS is associated with survival after cardiac arrest compared to other factors. POCUS can be used to to guide interventions outside of ACLS algorithms. POCUS may be used to identify patients where prolonged resuscitation efforts may not provide any benefit.
Variability in Interpretation of Cardiac Standstill Among Physician Sonographers Hu K, Gupta N, Teran F, Saul T, Nelson BP, Andrus P. Ann Emerg Med. 2018;71(2):193-198. DEEP DIVE SERIES Echo in Cardiac Arrest Objective - Do physicians among different specialties agree upon sonographic interpretation of cardiac standstill? Intervention - Clips of patients with cardiac standstill were shown to participants. They were then asked whether the clip shown displayed cardiac standstill and compared participant answers. Methods -127 faculty, fellows, and residents from separate specialties (Emergency Medicine, Critical Care, and Cardiology) surveyed Exclusion Criteria - unspecified specialty (14) or level of training (12) - no sonography experience (5) Primary Outcome: interpretation variability cardiac standstill • Moderate overall interrater agreement (α = 0.47) Secondary Outcomes: subgroup variability • Fellows - highest interrater agreement (α = 0.55) • Critical Care Physicians - lowest agreement (α = 0.40) N=127 Participants N=15 CC Attendings N=11 Fellows The Bottom Line There is a lack of agreement about what consists of cardiac standstill between physicians of different specialties and within the same specialty. This is likely attributable to the lack of a ubiquitous definition for cardiac standstill. Physicians would benefit from establishing common ground on this definition to determine which patients in cardiac arrest would benefit from further resuscitation efforts.
Lower-dose epinephrine administration and out-of-hospital cardiac arrest outcomes Fisk CA, Olsufka M, Yin L, et al. Resuscitation. 2018;124:43-48 DEEP DIVE SERIES Epinephrine in Cardiac Arrest Left Ventricular Compressions Improve Hemodynamics in a Swine Model of Out-of-Hospital Cardiac Arrest Anderson, KL, Castaneda, MG, Boudreau, SM, et al. Prehosp Emerg Care. 2017;21(2):272-280. DEEP DIVE SERIES Echo in Cardiac Arrest Objective - Does compression directly over the left ventricle (LV) improve hemodynamics and ROSC in swine model of cardiac arrest? Intervention - Echo was used to mark the location of the aortic root and the center of the LV. The animals were randomized to receive compressions on one of the two locations. Area of maximal compression during BLS was verified using TEE. Methods - Prospective, randomized comparative investigation Primary Outcome: coronary perfusion pressure (CPP) • Mean CPP was significantly higher in the LV group during 12-14 minutes interval of BLS and during minutes 22-30 of ACLS • Mean CPP of animals that attained ROSC > than mean CPP on non-ROSC animals Secondary Outcomes: • ROSCin LV group > ROSC in standard group • Aortic SBP/DBP in LV group > Aortic SBP/DBP in standard group • EtCO2 in LV group >EtCO2 in standard group • pH and PCO2 in LV group > pH and PCO2 in standard group Standard group N=13 ROSC N=0 Survival to 60 min N=0 LV group N= 13 ROSC N=9 Survival to 60 min N =9 The Bottom Line In swine model of cardiac arrest, chest compressions over the left ventricle improved hemodynamics and increased ROSC and survival to 60 minutes.
Lower-dose epinephrine administration and out-of-hospital cardiac arrest outcomes Fisk CA, Olsufka M, Yin L, et al. Resuscitation. 2018;124:43-48 DEEP DIVE SERIES Epinephrine in Cardiac Arrest Evaluation of out-of-hospital cardiac arrest using transesophageal echocardiography in the emergency department Teran F, Dean AJ, Centeno C, et al. Evaluation of out-of-hospital cardiac arrest using transesophageal echocardiography in the emergency department. Resuscitation. 2019;137:140-147. DEEP DIVE SERIES Echo in Cardiac Arrest Method - Single center, prospective, pragmatic, unblinded, observational study in a United States Urban emergency department Intervention - Transesophageal Echocardiography (TEE) during resuscitation of non-traumatic out-of-hospital cardiac arrest (OHCA) in adults - Four TEE views utilized for all subjects: Mid-esophageal 4 chamber view (ME4C), Mid-esophageal long axis view (MELAX), Trans-gastric short axis view (TGSAX) and Mid-esophageal Bicaval view). - Diagnostic information obtained intra-arrest via TEE reported by performing physician to resuscitation team leader Primary Outcome:The use of TEE during resuscitation of out-of-hospital cardiac arrest and in the immediate post-arrest period was found to have diagnostic, therapeutic, or prognostic clinical impact, defined by change in management, in 32 of 33 cases (97%). Secondary Outcomes: Feasibility: Mean door-to-TEE image acquisition time (n = 33) was 12 minutes, (Range 3-30 min. SD 8.16) CPR Quality: Location of Area of Maximal Compression (AMC) during CPR n = 17 n % Left Ventricle 8 47 Left Ventricular Outflow Tract or Aortic Root 9 53 Identification of Sonographic-ECG Rhythm Discrepancies n=33 n % Fine VF in patients thought to be in Asystole 4 12 Pseudo-PEA in patients thought to have CPR-indicating rhythms 2 6 Right Ventricular (RV) Dilation Study Incidence n = 13 (39%) ROSC was found to be a negative predictor of intra-arrest RV dilation, OD = 0.8 (p < 0.05 95% CI 0.006-0.82) The Bottom Line TEE can be initiated expeditiously in the setting of cardiac arrest resuscitation in emergency departments equipped for this imaging modality. This study also exemplifies the improved resolution and characterization of cardiac activity by TEE compared to cardiac and hemodynamic monitoring equipment routinely employed in the setting of cardiac arrest resuscitation, yielding management-changing diagnostic information in nearly all cases while also providing continuous visual feedback on CPR quality without interruption of chest compressions.
Transesophageal Echocardiography During Cardiopulmonary Resuscitation Is Associated With Shorter Compression Pauses Compared With Transthoracic Echocardiography Fair J, Mallin MP, Adler A, et al. Ann Emerg Med. 2019;73(6):610-616. DEEP DIVE SERIES Echo in Cardiac Arrest Objective - To compare the duration of chest compression pauses during pulse and rhythm checks when using transthoracic echocardiography, transesophageal echocardiography, or manual palpation during cardiac arrest resuscitations. Intervention - Pauses for pulse and rhythm checks during CPR were timed and compared when using TEE, TTE, and manual palpation. Methods - Retrospective analysis of video recordings of cardiopulmonary resuscitations. - 25 patients in cardiac arrest analyzed for a total of 136 pulse check CPR pauses - End point of CPR was either achievement of ROSC or declaration of death - Compressions were not paused for transesophageal insertion - Exclusion criteria: if procedures were performed (intubations, arterial line insertions, etc.) Primary Outcome: Time (in seconds) of pauses in chest compressions when performing TEE, TTE, or manual palpation for pulse and rhythm checks in CPR • Difference between TTE and TEE is 10 seconds (95% CI 5 to 14 seconds) • Difference between TEE and manual palpation is -2 seconds (95% CI -6 to 2 seconds) • Difference between TTE and manual palpation is 8 seconds (95% CI 4 to 11 seconds) The Bottom Line In the setting of cardiac arrest resuscitations, transesophageal echocardiography was associated with significantly shorter pauses during pulse and rhythm checks compared to transthoracic echocardiography and manual palpation.
Implementation of the Cardiac Arrest Sonographic Assessment (CASA) protocol for patients with cardiac arrest is associated with shorter CPR pulse checks Clattenburg EJ, Wroe PC, Gardner K, et al. Resuscitation. 2018;131:69-73. DEEP DIVE SERIES Echo in Cardiac Arrest Primary Outcome: Difference in CPR pulse check duration between the pre and post intervention period. Objective Can the CASA protocol reduce the duration of interruptions in CPR during resuscitation of cardiac arrest? Intervention Pre CASA intervention Non-traumatic CAs in ED= 129 Video taped= 38 Post CASA interventionNon-traumatic CAs in ED=58 Video taped= 45 The Bottom Line The implementation of a structured algorithm for ultrasound use during cardiac arrest significantly reduced the duration of CPR interruptions when ultrasound was performed. Methods Quasi -experimental pre and post intervention study.
The Right Ventricle Is Dilated During Resuscitation From Cardiac Arrest Caused by Hypovolemia: A Porcine Ultrasound Study Aagaard R, Granfeldt A, Bøtker MT, Mygind-Klausen T, Kirkegaard H, Løfgren B. Crit Care Med. 2017;45(9):e963-e970. DEEP DIVE SERIES Echo in Cardiac Arrest Objective -Dilation of the RV can occur during cardiac arrest due to the inherent physiology of arrest. This study aimed to assess the RV during cardiac arrest due to hypovolemia, hyperkalemia, and arrhythmia. Intervention • RV end-diastolic diameter was measured by transthoracic echo on pigs in cardiac arrest. Methods • 10 pigs were induced into hypovolemic cardiac arrest by controlled bleeding. • 10 pigs were induced into hyperkalemic cardiac arrest by the IV injection of potassium. • 10 pigs were induced into an arrhythmogenic cardiac arrest through electricity applied through a TVP. Primary Outcome The RV end-diastolic diameter was significantly larger in all three groups compared to the baseline, with hypovolemia having the largest increase. The diameter was not statistically different in the hyperkalemia and arrhythmia groups. The Bottom Line The RV can dilate naturally during cardiac arrest. Thus, RV dilation in itself during cardiac arrest cannot be used to justify therapeutic modalities such as lytics for pulmonary embolism.
Ultrasound use during cardiopulmonary resuscitation is associated with delays in chest compressions Huis In 't Veld MA, Allison MG, Bostick DS, et al. Resuscitation. 2017;119:95-98. DEEP DIVE SERIES Echo in Cardiac Arrest Objective To determine if transthoracic echo negatively affects CPR performance. Intervention -The duration of pulse checks was examined in those receiving a TTE during cardiac arrest vs those not receiving a POCUS. Methods • A prospective cohort study was performed. • Resuscitations were recorded where POCUS was utilized during pulse checks along with resuscitations where POCUS was not used. • A linear mixed model was used to determine the effect of POCUS on pulse checks. • Twenty-three patients were enrolled with 123 pulse checks performed. Primary Outcome: Length of Pulse Checks POCUS significantly increased the duration of a pulse check by 8.4s. 95% CI 6.7-10. P = <0.0001 The Bottom Line Ultrasound is a powerful tool in caring for the critically ill; however, it must be utilized in a way that does not overshadow interventions that have proven benefit (eg, chest compressions).
















