Download
1 / 27
570 likes | 1.59k Views
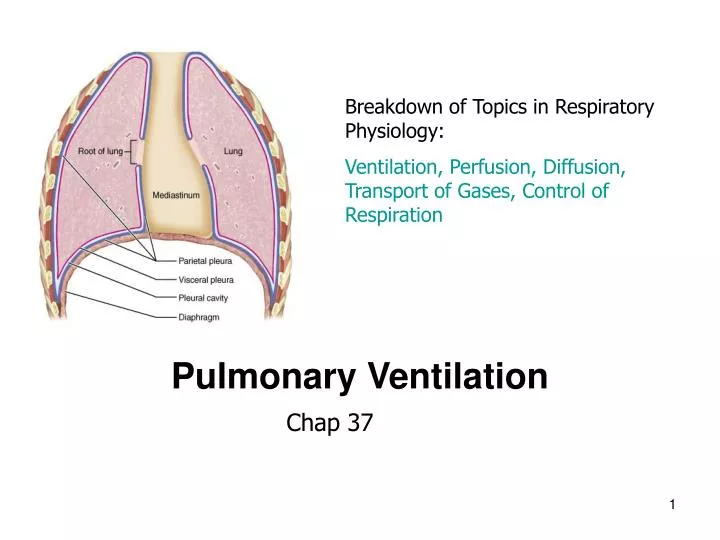
Breakdown of Topics in Respiratory Physiology: Ventilation, Perfusion, Diffusion, Transport of Gases, Control of Respiration. Pulmonary Ventilation. Chap 37. Functions of the Respiratory System. Respiration Acid-base balance Enabling vocalization

E N D
Breakdown of Topics in Respiratory Physiology: Ventilation, Perfusion, Diffusion, Transport of Gases, Control of Respiration Pulmonary Ventilation Chap 37
Functions of the Respiratory System • Respiration • Acid-base balance • Enabling vocalization • Defense against pathogens and foreign particles • Route for water and heat losses • Enhancing venous return • Activation of certain plasma proteins (e.g. Ang I)
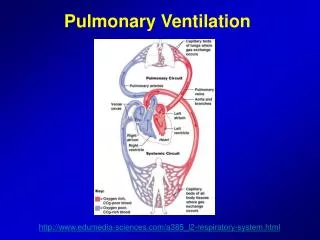
General Concepts of Respiration Respiratory System and CV System • Ventilate: bring the air to the blood • Gas exchange: diffusion, alveolar air with blood; get gases into/out of plasma water; to/from erythrocytes; to /from Hb • CV system: deliver gases to/from cells • O2 utilization: Mitochondria need the oxygen to metabolize fuels. (oxidative phosphorylation)
General Concepts: Airway Anatomy Surface area 70 sq meters- each lung! Barrier/ thickness to diffusion 0.2 microns Conductive airways vs. respiratory airways. Do you remember the difference?
Conducting zone: air passageway (anatomical dead space 150ml) Cartilage- support necessary to prevent collapse during inspiration due to decline in air pressure Bronchioles- no cartilage for support but do have elastic fibers-can change diameter! (increase or decrease resistance!) Terminal bronchioles Respiratory zone –air exchange. starts with respiratory bronchioles to alveolar ducts to alveolar sacs with alveoli
Ventilation Inspiration (inhalation) Expiration (exhalation) Normal inhalation, normal exhalation Forced inhalation, forced exhalation • Concepts: • Pressure gradient created by volume changes (Boyle’s Law) • Anatomy of lung and chest wall
Gas Laws Equation of State P V= n R T • P = gas pressure • V= gas volume • T= gas temperature (Kelvin scale) • N = number of moles of gas • R = universal gas constant Boyle's Law P1V1=P2V2 • Pressure and volume are inversely related (if other variables are kept constant.)
Gases move down pressure gradients P atm = 760 torr Flow Rule = Patm-Palv Resistance How are the pressure gradients changed? According to Boyle’s law we will need to create volume changes! PROBLEM! THE LUNGS ARE NOT MUSCULAR STRUCTURES! p alveolar = 758 torr Air moves from high to low pressure
Boyle’s Law If working with a closed system, a fixed number of gas molecules, and temperature is constant, then Pressure is inversely related to volume P = K V Or, in other words –changes in lung volume will lead to changes in pressure P V V P
Diaphragm Mechanics of Ventilation • Normal Inspiration • Is an active process (It’s work! ATP using) • Contract Diaphragm and it moves inferiorly to increase thoracic volume -60-75% of volume change • Contract external intercostals • Forced Inspiration • Accessory muscles needed • Sternocleidomastoid • Scalenes • Serratus anterior • Others (erector spinae)
When the chest wall moves, so do the lungs! Why are the lungs right up against the chest wall? • Pleural Space or Cavity • a vacuum (contains no air) • pleural fluid (water) has surface tension Result? Lung moves with the chest wall Lungs are not muscular organs, they cannot actively move. They move with the chest wall.
Mechanics of Ventilation • Normal Expiration- A Passive process • Simply relax the muscles of inspiration • Rely on the elastic properties of lung (like a balloon deflating on its own) • Forced Expiration • Relax muscles of inhalation AND • Contract internal intercostals • Contract Abdominal muscles • Internal and external obliques • Transverse abdominis • Rectus abdominis
Both the Lung and Chest Wall are Elastic • Both lung and chest wall have the tendency to recoil • What is recoil? Tendency to snap back to resting position (like a stretched rubber band recoils when youlet go of one end) The chest wall recoils outward (springs out) The lung recoils inward (ie. it collapses!)
expiration inspiration Palv=0 Palv (mmHg) Palv=+1 Palv=0 Palv=0 Palv= -1 0.5 Breath vol. (L) • Increase in lung volume decreases intra-alveolar pressure (we now have a pressure gradient) = air goes in. • Decrease in lung volume raises intra-alveolar pressure above atmosphere = air goes out.
Pressures First two create the pressure gradient that drives ventilation Atmospheric Pressures (Patm)- pressure of the outside air (760mmHg=760 torr = 1 atm). Intra-alveolar pressure (Palv) pressure within the alveoli of the lungs. Equal to Patm (0mmHg) at rest, but varies during phases of ventilation. Intra-pleural pressure – (Pip) pressure in the intra-pleural space. • Pressure is negative because of thelack of air in the intrapleural space, lymph drainage, and opposing forces of lung and chest wall. Transpulmonary (palv-Pip)
What happens if the lung dissociates from the chest wall? • Pneumothorax: air in the pleural cavity • Hemothorax: blood in the pleural cavity • How? • Injury (Gun shot, stabbing) • Spontaneous (tissue erosion, disease lung) • Bleeding wound • Chest wall recoils outward (barrel chest) • Lung recoils inward (atelectasis = alveolar, lung collapse)
P atm = 760 torr p alveolar = 758 torr Positive vs. Negative Pressure Breathing • Normally, the pressure gradient is produced by changing palv • This is called negative pressure breathing • If one changes patm, then this is positive pressure breathing • Ex. bag, cpr, mouth to mouth Air moves from high to low pressure Is this positive or negative pressure breathing?
Respiratory Cycle • A single cycle of inhalation and exhalation • Tidal volume: amount of air you move into or out of your lungs during a single respiratory cycle. • Respiratory rate: number of breaths per minute (12-18; children higher 18-20).
Rates: How much air moves in one minute? • Total Ventilation: Minute Ventilation Volume (MVV) • Tidal volume x respiratory rate • Alveolar Ventilation • (Tidal volume-dead space) x respiratory rate
Definitions of Dead Space Anatomic Dead Space Physiologic Dead Space Low Blood Flow “Deadspace”: a volume of air that is not involved in gas exchange with blood • Anatomical dead space volume (based on size of one’s conductive airways) • Typically about 150 ml • Physiological dead space volume (anatomical dead space plus any areas of lung where alveoli are not perfused with blood) • Depends on ventilation-perfusion ratio • But also, in disease, depends on blocked arteries
Alveolar Ventilation vs. Total Minute Ventilation of the lung Total ventilation rateis the volume of air that enters the airways (passes the lips) each min. Total ventilation = Tidal volume x rate of breathing = (500 ml/breath) x 12 breaths/min = 6,000 ml/min Alveolar ventilation is the volume of air that fills all the lung’s respiratory airways (alveoli) each min. In a normal, healthy lung, this might be: Alveolar ventilation = (tidal volume – dead space volume) x rate of breathing = (500 ml/breath – 150 ml) x 12 breaths/min = (350 ml/breath) x 12 breath/ min = 4, 200 ml/min In a diseased, poorly perfused lung, this value may well be much lower. Then, is panting an example of hyper, normal, or hypoventilation????
Lung function tests • Lung volumes are assessed by spirometry. • Subject breathes into a closed system in which air is trapped within a bell floating in H20. • The bell moves up when the subject exhales and down when the subject inhales. • Spirometry • Static lung tests • Volumes and capacities • No element of time involved, ie. How long does it take you to push the air out? Normal expiration takes 2-3 x longer than inspiration • Dynamic lung tests • Time element, rate of exhale • How much, how quickly?
Static Lung Tests Pulmonary Volumes 3500ml 4600ml 6000ml 3100ml 500ml 2400ml 1200ml 1200ml Figure 37-6; Guyton & Hall
Residual Volume (* can’t be exhaled, requires indirect measurements, not simple spirometry) Capacities are two or more volumes added together
Forced Vital Capacity (FVC, FEV 1.0) Dynamic Lung Tests
Obstructive Disease: Decreased VC Increased TLC, RV, FRC. FEV1/VC is less than 80% Restrictive Disease: Decreased VC Decreased TLC, RV, FRC So FEV1/VC ratio normal Lung Capacity and Disease— Summary • FRC: ERV +RV. Why is this important? • It’s the volume of air in your lungs at the end of a normal exhale. • It represents the normal equilibrium position of your chest wall trying to spring out and lung to recoil, but forced together due to pleural cavity.