Download
1 / 37
410 likes | 532 Views
This comprehensive guide covers the diagnosis and treatment of Polycystic Ovary Syndrome (PCOS), including diagnostic criteria, PCOS phenotypes, and treatment options such as ovulation induction. Understand the complexities of PCOS diagnosis, the impact of hyperandrogenemia, and the role of polycystic ovaries in the condition. Learn about revised diagnostic criteria, exclusion of other causes, and normative data challenges in PCOS diagnosis. The text explores ovulation induction methods, including Clomiphene Citrate and Metformin, and addresses the impact of obesity on PCOS features. Discover the latest research on PCOS treatment and gain insights into optimizing fertility and managing PCOS symptoms effectively.

E N D
Diagnosis and Treatment of PCOS Nick Macklon University Medical Centre Utrecht The Netherlands
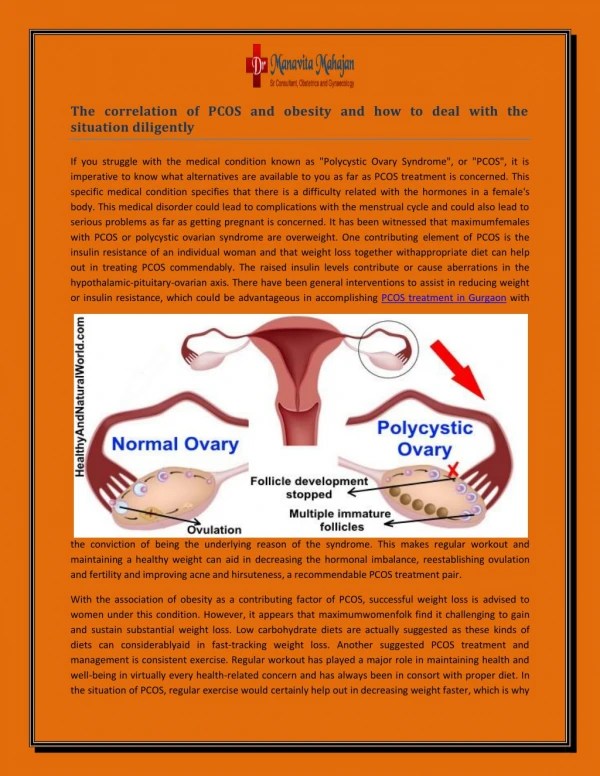
PCOS- diagnostic dilemma’s - • Endocrine features • high androgens • high LH • insulin resistance • Clinical features • hirsutism • obesity • anovulation • Polycystic ovaries • increased follicle # • increased stroma • increased ovarian volume
PCOS diagnosis- 1990 NIH criteria - Hyperandrogenemia PCOS Chronic anovulation
Epidemiology of PCOS Population/ethnicity sample size PCOS reference Greek Island, Lesbos 192 NIH Diamanti, JCEM 99 17-45 yrs 6.8% Caucasian, reproductive age 154 NIH Asuncion, JCEM 00 Blood donors, Spain 6.5% Preemployment physical, US 400 NIH Azziz, JCEM 04 18-45 yrs (223 black, 166 white) 6.6% Knochenhauer, JCEM 98
Why Revisit the NIH Criteria? • First step to standardizing diagnosis • Based on Questionnaire • PCOS -broader spectrum of ovarian dysfunction • -regular cycles and hyperandrogenism and/or PCO • -PCO without hyperandrogenism • May not be suitable for trials of clinical outcomes
ESHRE / ASRM endorsed PCOS Consensus MeetingRotterdam, The Netherlands Azziz Laven Bouchard Dewailly Legro Dahlgren Homburg Wild Norman Franks Nestler Diamanti Pasquali Ibanez Balen Taylor Pugeat Filicori Magoffin Fauser Tarlatzis Wild Tan Dunaif Devoto Strauss Rotterdam, May 2003
Revised Diagnostic Criteria for PCOS 1999 NIH Criteria (both 1 and 2) 1. Chronic anovulation 2. Clinical and/or biochemical signs of hyperandrogenism Exclusion of other aetiologies Revised 2003 Rotterdam Criteria (2 and of 3) 1. Oligo- and/or anovulation 2. Clinical and/or biochemical signs of hyperandrogenism 3. Polycystic ovaries Exclusion of other aetiologies
PCOS diagnostic criteria • Exclusion of other causes of androgen excess • Cushing, 21 hydroxylase deficiency • androgen producing tumours • Exclusion of other causes of anovulation • Hypogonadotropic hypogonadism • Premature ovarian failure • Hyperprolactinaemia • Often obesity (but not required) • Often elevated LH (but not required) • Often hyperinsulinemia (but not required)
Normative data lacking Subjective May be less prevalent in East Asian Women Variable laboratory methods Wide variability in normal population Normative ranges not well established in well characterized control populations PCOS- hyperandrogenemia - • Clinical: • Acne • Hirsutism • Biochemical: • Testosteronetotal or free (unbound) • Free androgen index(T x 100 / SHBG) • Androstenedione? • DHEAS? • combination
Balen, HRU 2003 PCOS- polycystic ovaries - • Presence of 12 or more follicles (2-9mm) per ovary. Location not important. • Ovarian volume >10mls • 0.5 x length x width x thickness • Ovarian stroma objective? • One ovary sufficient for diagnosis • Scan early follicular phase
1 PCOS Hyperandrogenemia Oligo/anovulation (WHO 2 type) PCO
PCOS phenotypes NIH Rotterdam additions Oligo/anovulation + + + Hyperandrogenemia + + + PCO + + +
Ovulation Induction Type of ovarian stimulation aimed at restoring normal fertility by inducing single dominant follicle selection, ovulation and hence normo-ovulatory cycles.
Ovulatory infertility and Obesity Mulders et al. Hum Reprod Update 2003
Impact of obesity of clinical, hormonal and metabolic features of PCOS Hoeger K, Clin Obstet Gynecol, 2007
Treatment Controls Ovulation Induction (Guzick et al., Fertil Steril, 1994) Step 1: Lose weight SHBG SHBG - T Insuline Glucose Total T 90 .9 16 90 120 80 .8 14 80 110 70 .7 12 70 100 60 .6 10 60 90 50 .5 8 50 40 .4 6 40 Pre Post Pre Post Pre Post Pre Post Pre Post
Ovulation Induction Step 2: Clomiphene Citrate • Non-steroidal estrogen antagonist • Blocks negative feedback of E2 at pituitary • 50-150mg from day 2-5 of cycle • FSH 50-60% • 70-80% ovulate • 22% conception rate per cycle • Cheap & effective
Ovulation Induction Step 3: Metformin? Step 3: Aromatase inhibitors? Step 3: Electrocautery of ovaries? Step 3: Gonadotropins?
Ovulation Induction Step 3: Add Metformin? 626 womenwith PCOS Combination of metformin and CC 50-150mg CC plus placebo from cycle day 3-7 500 mg-2000 mg Metformin plus placebo • Up to 6 months treatment • Obesity not an exclusion Legro et al, NEJM
Ovulation Induction Step 3: Add Metformin? Legro et al, NEJM 2007
Ovulation Induction Step 3: Add Metformin? Tarlatzis etal, Hum Rep 2007
ER ER ER ER E2 FSH Day 10 Aromatase Inhibitors ER ER ER ER E2 FSH AI Day 5 Halflife: 45-48 hours
Aromatase Inhibitors Outstanding questions • Impact of low intrafollicular estradiol levels? • Impact of intrafollicular androgen accumulation? • : positive (via increase in FSH receptors) • : negative: androgen excess • Impact on oocyte quality? • Few RCTS: Badawy et al; No advantage over CC • Teratogenicity issues?
STEP-UP Protocol hCG FSH levels FSH dose STEP-DOWN Protocol FSH levels hCG FSHdose Gonadotropin regimens window 10mm menses
Cumulative pregnancy rates after ovulation induction 1 0.8 0.6 Ongoing Singleton Pregnancy Rate Resulting in Live Birth 0.4 0.2 0 0 3 6 9 12 15 18 21 24 Follow-up (months) Eikemans et al, Hum Reprod 2003
Ovulation Induction Step 3: Electrocautery of ovaries
FSH / HMG GnRH antag IVF in PCOS: Ovarian Stimulation The ‘classical’ long protocol hCG FSH / HMG Luteal support OC GnRH agonist The ‘antagonist’ protocol hCG/GnRHa Luteal support Cycle day 1
IVF outcomes in women with PCOS (458) vs Controls (694) A meta-analysis. Heijnen et al, Hum Reprod Update, 2006 WMD for number oocytes per ovum pick up WMD for number of oocytes fertilised OR for chance of cancellation OR for chance of live birth per started cycle OR for chance of miscarriage per started cycle
Pregnancy outcomes in PCOS Meta-analysis: 720 women with PCOS vs 4505 controls OR 95% CI Gestational Diabetes: 2.94 1.70-5.08 Pregnancy induced hypertension: 3.67 1.98-6.81 Pre-eclampsia 3.47 1.95-6.17 Pre-term birth 1.75 1.16-2.62 Peri-natal mortality 3.07 1.03-9.21
Conclusions • Need for uniform definition • Lifestyle as therapy • Clomiphene still first line? • Gonadotropins versus Laparoscopic electrocautery? • Ovulation Induction works! • IVF effective- and with appropriate care: safe • Role of in-vitro oocyte maturation?