Download
1 / 10
130 likes | 186 Views
β – ADRENERGIC BLOCKERS. β -Adrenergic blockers All are competitive antagonists at β receptor. Classification ISA MSA ( Partial agonist ) I) Nonselective ( β 1 β 2 ) Alprenolol, oxprenolol + + Propranolol - + Pindolol + -

E N D
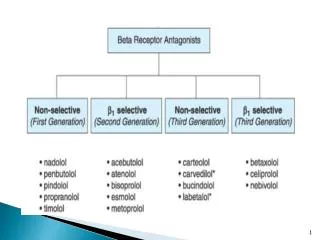
β -Adrenergic blockers All are competitive antagonists at β receptor. Classification ISA MSA ( Partial agonist ) I) Nonselective (β1β2 ) • Alprenolol, oxprenolol + + • Propranolol - + • Pindolol + - • Sotalol, Timolol, Nadolol - - Nonselective with additional α– blocking action Labetalol - + Carvedilol + II) Cardioselective (β1) • Acebutolol + + • Metoprolol, Esmolol - - Betaxolol, Atenolol
III) β2– Selective blocker- Butoxamine ( only used for research purpose ) IV) β1 Selective – β blocker with β2 agonistic activity Celiprolol + - Pharmacological actions Heart – block β1 receptors force of contraction C.O. H.R Conduction across A-V node refractory period Decrease oxygen requirement Decrease automaticity
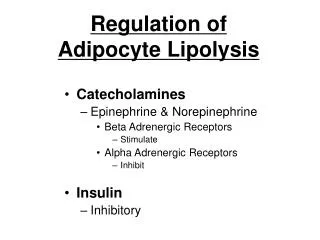
Blood vessels • No direct action • P.R. may increase initially dlt. Blockade of β2 mediated vasodilatation • On prolonged administration –P.R. es. Blood pressure B.P = C. O X P.R Decrease in B.P a) Decrease C.O by blocking β1 receptors present on heart. b) Decrease in P.R. c) Decrease release of NE from adrenergic neurons peripherally d) Decrease central symp- outflow e) Decrease renin release by blocking β1 receptors present on JG apparatus. f) Parse mild vasodilatory action
Respiratory tract Block β2 receptors present on tracheal bronchial tree. Bronchoconstriction Metabolic Inhibit glycogenolysis TG levels Eye- Decrease aqueous humor secretion Adverse effects CNS- excessive dreaming Nightmares RS- Bronchial asthma CVS- Myocardial insufficiency –CCF –dlt block of sympathetic support to the heart. Bradycardia Partial, complete heart block Exacerbates variant angina
Metabolic – Lipid - Increase TG. LDL, Decrease HDL- risk of coronary artery atherosclerosis CHO- CI in Diabetes mellitus Decrease exercise capacity Worsening of PVD Rapid withdrawal- Rebound hypertension Supersesitivity Anginal attacks of β receptors Arrhythmias Β1 selective blockers Bronchial asthma Diabetes mellitus Peripheral vascular disease No effect on Lipid profile Exercise capacity not affected
β blockers with intrinsic symptomimitic action Less bradycardia Less cardiac depression – in patients with poor cardiac reserve Withdrawal –less likely the phenomena of supersensitivity Plasma lipid profile – Not affected Contraindications Bronchial asthma Diabetes mellitus Hearts rate < 45 / min Heart block Variant angina Drug INTERACTIONS • Should never be combined with calcium channel blockers like verapamil • Delays recovery from hypoglycemia due to insulin. Oral antidiabetic agents .
Atenolol Propranolol 1) Selective β1 blocker Nonselective (β1 + β2 ) 2) No membrane stabilizing + 3) Less 1st pass effect significant 1st pass effect 4) Low lipid solubility Lipid solubility +++ 5) CNS Penetration - ed + Less CNS S/E 6) Longer duration of action short duration of action 7) Frequency administration Four times a day Once a day 8) Renal elimination Hepatic elimination
THERAPEUTIC USES OF BETA BLOCKERS 1.Hypertension Atenolol – 50-100 mg OD Propranolol -40 – 160 mg / day 2. Angina Pectoris - Ve onotropic , chronotropic effect Decrease in C.O Decrease in O2 requirement of Heart O2 demand = O2 supply 3. Cardiac arrhythmias – decrease automaticity of ectopic pacemakers decrease conduction through A-V node decrease refractory period of A-V node Used in supraventricular arrhythmias 4. Myocardial infarction Limit infarct size by decreasing O2 demand Myocardial Salvage
B) Prevent arrhythmias Prophylaxis To prevent re infarction mortality 5.Congestive cardiac failure Endocrine uses • Hyperthyrodism • Pheochromocytoma CNS USES 1. Chronic prophylaxis of Migraine Propranolol 2. Essential tremors 3. Anxiety - Palpitations,tremors 4. Glaucoma- Timolol -0.25 -0.5% Betaxolol , Levobunolol Decreases aq. humour seccretion Wide angle glaucoma. Portal Hypertension