Download
1 / 11
110 likes | 279 Views
Choice of Antibiotics in Diverticulitis. Jeff Poynter University of Michigan Medical School. The Problem: Uncomplicated Diverticulitis.

E N D
Choice of Antibiotics in Diverticulitis Jeff Poynter University of Michigan Medical School
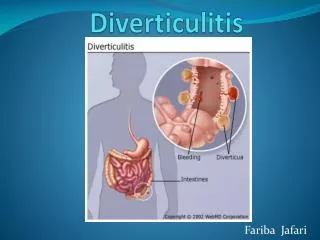
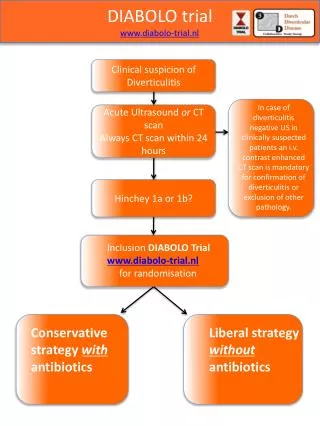
The Problem: Uncomplicated Diverticulitis • Uncomplicated diverticulitis represents a localized infection, primarily by Gram-negative rods and anaerobes, mostly E. coli and B. fragilis. (Ambrosetti P, et al.) • Conservative (medical) treatment of acute uncomplicated diverticulitis is successful in 70-100% of patients. (Janes, et al. and Detry, et al.)
Some Common Choices of Antibiotics: Dual-Agent Coverage • Quinolone with metronidazole (Ciprofloxacin, 500 mg PO BID plus metronidazole, 500 mg PO BID) • Ciprofloxacin 400 mg IV q 12 hours plus metronidazole 500 mg PO/IV q 6-8 hours • Levofloxacin 500 mg IV daily plus metronidazole 500 mg PO/IV q 6-8 hours • Choices made in part with regard to history of drug allergies
Some Common Choices of Antibiotics: Single-Agent Therapy • Amoxicillin-clavulanate 875/125 mg PO BID • Ampicillin-sulbactam 3 g IV q 6 hours • Piperacillin-tazobactam 3.375 or 4.5 g IV q 6 hours • Ticarcillin-clavulanate 3.1 g IV q 4 hours • Imipenem 500 mg IV q 6 hours • Meropenem 1 g IV q 8 hours
Single- versus Dual-Antibiotic Therapy • Single and multiple antibiotic regimens are equally effective as long as both Gram-negative rods and anaerobes are covered adequately. (Kellum, et al.)
The Problem: Complicated Diverticulitis • Complications include obstruction, abscess formation, fistula formation or perforation. • Requires IV antibiotics plus surgery (usually Hartmann operation).
Antibiotics in Complicated Diverticulitis • Ampicillin 2 g IV q 6 hours plus gentamicin 1.5-2.0 g IV q 8 hours plus metronidazole 500 mg IV q 8 hours • Imipenem/cilastin 500 mg IV q 6 hours • Piperacillin-tazobactam 3.375 mg IV q 6 hours • Moxifloxacin • Tigecycline, a new drug, has recently been approved for the treatment of intra-abdominal infections; it has not been shown to be superior to the traditional regimens. • Lots of choices- the goal is to cover GNRs and anaerobes and proceed to definitive surgery. No single regimen has been shown to be definitely superior to the others.
Krobot K, et al • 425 patients who required surgery for community-acquired secondary peritonitis, including patients with complicated diverticulitis. • 13% of patients did not receive appropriate antibiotics, defined as not covering all bacteria later isolated or not empirically covering typical aerobic and anaerobic organisms in the absence of culture results. • 26% of appropriately treated patients and 30% of inappropriately treated patients had colonic sources of infection. • Resolution of infection with initial or step-down therapy after primary surgery was significantly less likely to occur (53% vs. 79%). • Failure of resolution of infection due to inadequate choice of antibiotics resulted in six-day prolongation of stay in hospital (20 versus 14 days total).
Schechter S, et al • Survey of 373 Fellows of the American Society of Colon and Rectal Surgeons surveyed regarding diagnosis and treatment of acute uncomplicated diverticulitis • Half of responders chose a single-drug regimen: second-generation cephalosporin (27%) or ampicillin/sulbactam (16%). • Single-therapy oral antibiotics at discharge were ciprofloxacin (18%), amoxicillin/clavulanate (14%), metronidazole (7%) and doxycycline (6%). • Combinations chosen were ciprofloxacin/metronidazole (28%) and TMP-SMX/metronidazole (6%). 21% chose various other antibiotics.
Summary • Antibiotic coverage must cover both Gram-negative rods and anaerobes, or infections will persist longer and prolong length of stay in hospital. • Single or multiple antibiotic regimens are equally effective as long as coverage is adequate- this equivalency amongst choices is probably why there aren’t any recent studies attempting to identify superior drugs! • Top choices by ASCRS Fellows include: ciprofloxacin plus metronidazole, ciprofloxacin alone and amoxicillin/clavulanate. • The dominant consideration regarding choice of antibiotics is coverage of GNRs and anaerobes!
References • Krobot K, et al. Eur J Clin Microbiol Infect Dis 2004 Sep;23(9):682-7. • Papi C, et al. Aliment Pharmacol Ther 9:33-39. • Schechter S, et al. Dis Colon Rectum 1999; 42:470. • Up-to-Date, “Diverticulitis”. • Imbembo, AL, Bailey, RW. Diverticular disease of the colon. In: Textbook of Surgery, 14th ed, Sabiston, DC Jr (Ed), Churchill Livingstone 1992. p.910. • Rafferty, J, Shellito, P, Hyman, NH, Buie, WD. Practice parameters for sigmoid diverticulitis. Dis Colon Rectum 2006; 49:939. • Ambrosetti P, et al. Dis Colon Rectum 2000; 43:1363-7. • Janes S, et al. Br J Surg 2005; 92:133-42. • Detry R, et al. Int J Colorectal Dis 1992; 7:38-42. • Kellum JM, et al. Clin Ther 1992; 14:376-84. • Solomkin JS, et al. Clin Infect Dis; 37(8): 997-1005. • Goldstein EJ, et al: In vitro activity of moxifloxacin against 923 anaerobes isolated from human intra-abdominal infections. Antimicrob Agents Chemother 50. (1): 148-155.2006. • Olivia ME, et al: A multicenter trial of the efficacy and safety of tigecycline versus imipenem/cilastatin in patients with complicated intra-abdominal infections. BMC Infect Dis 5. 88.2005.