Download
1 / 11
110 likes | 241 Views
Design of Phase III Microbicide Trials: Choice of Control Group August 20, 2003. Rosalie Dominik, DrPH Director of Biostatistics Institute for Family Health Family Health International. n-9 HIV/STI Research in Cameroon. Observational study of n-9 suppositories

E N D
Design of Phase III Microbicide Trials: Choice of Control GroupAugust 20, 2003 Rosalie Dominik, DrPH Director of Biostatistics Institute for Family Health Family Health International
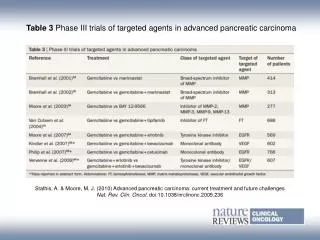
n-9 HIV/STI Research in Cameroon • Observational study of n-9 suppositories • Zekeng et. al., AIDS 1993; 7(5): 725-731. • Blinded randomized controlled trial (RCT) of n-9 film versus placebo film control • Roddy et al., N Engl J Med 1998; 339:504-510. • Unblinded RCT of n-9 gel versus condom-only control • Roddy et al., JAMA 2002; 287:1117-1122.
Potential Labeling? Use of MICROBICIDEGel reduces a woman’s risk of HIV infection during vaginal intercourse. • To best protect against the risk of HIV infection during vaginal intercourse, use a condom during every act of intercourse. • Use of MICROBICIDEGel provides additional or back-up protection against HIV infection.
Primary Question of Interest • Does use of the microbicide formulation reduce the risk of HIV acquisition compared to non-use, holding all other risk factors constant • Gold standard : Blinded RCT of microbicide gel versus a truly inactive placebo • Use ‘best available’ placebo
Microbicide vs Condom-Only • Those assigned to condom-only know they don’t have the potential protection that the microbicide might provide • Motivation to use condoms or to avoid risky acts would not be the same in the two groups • Choices to be made differ, and so behaviors will likely differ. • Microbicide Arm: • Gel + Condoms (As counseled) • Gel Alone • Condoms Alone • Nothing • Condom-Only Arm: • Condoms (As counseled) • Nothing
Example 1: Increased Chance of Missing a Protective Effect • Assume condoms reduce risk by 95% when used • Assume that microbicide reduces HIV risk by 50%compared to true placebo but that a condom-only control arm will be included • Design study to have ~90%power to detect a 50% reduction (alpha=.05, 2-sided) • If condom use is truly 65% in microbicide arm and 75% in the condom-only arm, study will have ~50%power to conclude microbicide provides protection
Example 1 (continued) • Assume that microbicide reduces HIV risk by 50% compared to true placebo but that a condom-only control arm will be included • If condom use is truly 80% in microbicide arm and 90% in condom-only arm, study will have ~15%power to find protective effect • and, ~20% chance of seeing more HIV infections in the microbicide arm than in the condom only arm!
Example 1: Conclusion • Concern: Requiring a study that shows significantly fewer infections in a microbicide arm vs condom-only arm could lead to failure to promptly identify a product that protects against HIV.
Example 2: Increased Chance of False Positive Finding • Now assume that microbicide truly has no effect on HIV risk compared to a true placebo but that a condom-only control arm will be included • If condom use is truly 90% in microbicide arm and 80% in condom-only arm, ~65%chance of falsely concluding that the microbicide provides a protective effect (as compared to the 2.5%chance of a type I error in this direction when behaviors are balanced)
Placebo vs Condom Only • May provide evidence that ‘placebo’ actually protects against HIV • If we assume that condom only arm will use condoms at least as much as the placebo arm • and we see significantly fewer HIV infections in the placebo arm.
Conclusion • What we most want to know is ‘does use of the microbicide reduce the risk of HIV acquisition?’. • A blinded two-arm trial of a microbicide versus the best available placebo can provide sufficient evidence to support a claim that use of a new microbicide can reduce the risk of HIV acquisition.