Download
1 / 82
820 likes | 1.02k Views
Medical Immunology Immunobiology of HIV infection Jan 10, 2013. Keith Fowke 539 BMSB 789-3818 fowkekr@cc.umanitoba.ca. Medical Immunology IMed 7190. Topic: HIV resistance Lecturer: Keith Fowke Objectives: To discuss why HIV induces immune suppression

E N D
Medical Immunology Immunobiology of HIV infectionJan 10, 2013 Keith Fowke 539 BMSB 789-3818 fowkekr@cc.umanitoba.ca
Medical Immunology IMed 7190 • Topic: HIV resistance • Lecturer: Keith Fowke • Objectives: • To discuss why HIV induces immune suppression • To discuss why some individuals are resistant to infection • Expectations: • To list two main hypotheses why HIV infection leads to AIDS • To discuss the immunological and non-immunological methods of resistance to HIV infection
Outline Epidemiology of the disease HIV Disease HIV replication Why does HIV cause immunodeficiency? What does the CD4+ T cell do? Three types of T-helper cell. How does HIV decrease CD4+ levels? Apoptosis in HIV infection HIV Resistance Mechanisms of Resistance
Adults and children estimated to be living with HIV 2010 Eastern Europe & Central Asia 1.5 million [1.3 million – 1.7 million] Western & Central Europe 840 000 [770 000 – 930 000] North America 1.3 million [1.0 million – 1.9 million] East Asia 790 000 [580 000 – 1.1 million] Middle East&North Africa 470 000 [350 000 – 570 000] Caribbean 200 000 [170 000 – 220 000] South & South-East Asia 4.0 million [3.6 million – 4.5 million] Sub-Saharan Africa 22.9 million [21.6 million – 24.1 million] Latin America 1.5 million [1.2 million – 1.7 million] Oceania 54 000 [48 000 – 62 000] Total: 34.0 million[31.6 million – 35.2 million]
Estimated number of adults and children newly infected with HIV 2010 Eastern Europe & Central Asia 160 000 [110 000 – 200 000] Western & Central Europe 30 000 [22 000 – 39 000] North America 58 000 [24 000 – 130 000] East Asia 88 000 [48 000 – 160 000] ~7,400 people HIV infected daily Middle East&North Africa 59 000 [40 000 – 73 000] Caribbean 12 000 [9400 – 17 000] South & South-East Asia 270 000 [230 000 – 340 000] ~300 infected during this talk Sub-Saharan Africa 1.9 million [1.7 million – 2.1 million] Latin America 100 000 [73 000 – 140 000] Oceania 3300 [2400 – 4200] Total: 2.7 million [2.4 million – 2.9 million]
Estimated adult and child deaths from AIDS 2010 Eastern Europe & Central Asia 90 000 [74 000 – 110 000] Western & Central Europe 9900 [8900 – 11 000] North America 20 000 [16 000 – 27 000] East Asia 56 000 [40 000 – 76 000] ~4,900 people die daily ~200 die during this talk Middle East & North Africa 35 000 [25 000 – 42 000] Caribbean 9000 [6900 – 12 000] South & South-East Asia 250 000 [210 000 – 280 000] Sub-Saharan Africa 1.2 million [1.1 million – 1.4 million] Latin America 67 000 [45 000 – 92 000] Oceania 1600 [1200 – 2000] Total: 1.8 million [1.6 million – 1.9 million]
2008: 65,000 people living with HIV in Canada PHAC: Estimates of HIV Prevalence and Incidence in Canada, 2008
Annual Number of Individuals Testing HIV Antibody Positive 1985-2008 in Manitoba In 2011 there are more than 1100 people in HIV Care in Manitoba Manitoba Health & Healthy Living Statistical Update on HIV/AIDS January 1985 –December 2007 (http://www.gov.mb.ca/health/publichealth/cdc/surveillance/dec2007.pdf)
HIV in Manitoba 95 New Cases in 2011 Source: Manitoba HIV Program 2012 Report
Outline Epidemiology of the disease HIV Disease HIV replication Why does HIV cause immunodeficiency? What does the CD4+ T cell do? Three types of T-helper cell. How does HIV decrease CD4+ levels? Apoptosis in HIV infection HIV Resistance Mechanisms of Resistance
A diagnosis of AIDS is made whenever a person is HIV positive and: he or she has a CD4+ cell count <200 cells/µL, or his or her CD4+ cells account for <14% of all lymphocytes, or that person has been diagnosed with one or more of the AIDS-defining illnesses listed below. AIDS-defining illnesses: Candidiasis of bronchi, trachea, or lungs Candidiasis, esophageal Cervical cancer, invasive* Coccidioidomycosis, disseminated Cryptococcosis, extrapulmonary Cryptosporidiosis, chronic intestinal (>1-month duration) Cytomegalovirus disease (other than liver, spleen, or lymph nodes) Cytomegalovirus retinitis (with loss of vision) Encephalopathy, HIV related# (see Dementia) Herpes simplex: chronic ulcer(s) (>1-month duration) or bronchitis, pneumonitis, or esophagitis Histoplasmosis, disseminated Isosporiasis, chronic intestinal (>1-month duration) Kaposi sarcoma Lymphoma, Burkitt Lymphoma, immunoblastic Lymphoma, primary, of brain (primary central nervous system lymphoma) Mycobacterium avium complex or disease caused by M kansasii, disseminated Disease caused by Mycobacterium tuberculosis, any site (pulmonary*or extrapulmonary#) Disease caused by Mycobacterium, other species, or unidentified species, disseminated Pneumocystis jiroveci (formerly carinii) pneumonia Pneumonia, recurrent* Progressive multifocal leukoencephalopathy Salmonella septicemia, recurrent Toxoplasmosis of brain (encephalitis) Wasting syndrome caused by HIV infection# Additional illnesses that are AIDS defining in children, but not adults Multiple, recurrent bacterial infections# Lymphoid interstitial pneumonia/pulmonary lymphoid hyperplasia
Peterlin et al Nature Reviews Immunol 3; 97-107 (2003) HIV Genes and Proteins
HIV Structure exhiv.chat.ru
HIV Life Cycle • HIV enters via CD4 • RNA reverse transcribed into DNA • DNA integrates into host genome • Latency? • Replication produces proteins • Proteins assemble into new viruses Peterlin et al Nature Reviews Immunol 3; 97-107 (2003)
Treating HIV Infection • Three main sites for HIV drugs • Reverse transcriptase • HIV protease • HIV entry • Integration C. B. A. • Main classes of HIV drugs • Nucleoside analogues (zidovudine) - A • Non-nucleoside (nevaripine) - A • Protease Inhibitors (indinavir) - B • Chemokine Receptor Antagonists (maraviroc) – C • Fusion Inhibitors – (enfuvirtide) - C • Integrase Inhibitors - (elvitegravir) - D D. Peterlin et al Nature Reviews Immunol 3; 97-107 (2003)
Role of DCs in HIV Infection Nature Reviews Immunology2; 957-965 (2002)
The Kinetics of HIV Disease Progression Acute Phase Asymptomatic Phase AIDS 12 10 CD4+ T cells 8 HIV CTL Relative Values 6 Death Neut Ab 4 HIV viralload 2 0 0 1 3 6 12 24 36 48 60 72 84 96 108 120 132 144 Time Post Infection (Months) Alimonti, Ball & Fowke, J GenVirol (in press)
Outline Epidemiology of the disease HIV Disease HIV replication Why does HIV cause immunodeficiency? What does the CD4+ T cell do? Three types of T-helper cell. How does HIV decrease CD4+ levels? Apoptosis in HIV infection HIV Resistance Mechanisms of Resistance
Hallmark of HIV disease • Loss of CD4+ T cells from peripheral blood What is the role of CD4+ T cells in the immune response?
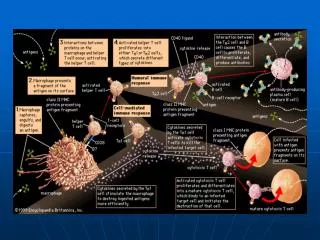
Subsets of CD4+ T helper cells Th17 Naive CD4+ Tcell APC+Ag T reg Activated CD4+ Tcell IL-4 IL-2 g IFN- IL-12 IL-4 Suppression g IFN- Th1 Th2 IL-4, IL-10 IL-4 IL-13 g IFN- IL-5 Dominant Cellular Dominant Humoral Immunity Immunity
The Kinetics of HIV Disease Progression Acute Phase Asymptomatic Phase AIDS 12 10 CD4+ T cells 8 HIV CTL Relative Values 6 Death Neut Ab 4 HIV viralload 2 0 0 1 3 6 12 24 36 48 60 72 84 96 108 120 132 144 Time Post Infection (Months) Alimonti, Ball & Fowke, J GenVirol (in press)
Mechanisms for CD4+ cell decline • Direct • Synctia formation (cell-cell fusion) • Direct viral cytopathic effect • Indirect • Apoptosis/PCD • Activation Induced Cell Death • Autoimmune mechanisms • Homology of viral proteins to self antigens • Superantigen-mediated deletion • Viral proteins acting as superantigens • Type 1/Type 2 cytokine dysregulation
Detection of Apoptosis CD4 APC CD8 CD4 12.3 8.2 9.2 0 Time 0 hrs 79.5 0 90.8 0 CD4 CD8 25.8 0 28.3 49.5 Time 6 hrs 74.2 0 22.2 0
Apoptosis in HIV infection • Mechanisms: • gp120/41 - CD4 crosslinking, ↓ BCL-2, ↑CD95(Fas)/CD95L(FasL) • gp120 induction of syncytia • HIV protease activates caspase 8 and ↓ BCL-2 • Tat – ↑ Caspase 8, Fas, FasL and ↓BCL-2 • Vpr – membrane disruption of mitochondrion • Nef - myristylated N-terminus interacts with TCR and leads to upregulation of Fas/L • Fas/FasL – altered in T cells and monocytes due to nef • AICD – increased Fas/FasL
CD4’s Role in Signal transduction T-Cell Activation
Uninfected CD4 T cell CD4 cross-linking activates lck gp120-induced CD4-crosslinking = CD4 =sgp120 =p56lck =P-p56lck ↑ CD95(Fas) ↓ BCL-2 apoptosis
HIV nef effects on CD4 and MHC I Peterlin et al Nature Reviews Immunol 3; 97-107 (2003)
Outline Epidemiology of the disease HIV Disease HIV replication Why does HIV cause immunodeficiency? What does the CD4+ T cell do? Three types of T-helper cell. How does HIV decrease CD4+ levels? Apoptosis in HIV infection HIV Resistance Mechanisms of Resistance
Kisumu Nairobi Kenya Nairobi • HIV prevalence • 14% in 1997 • 6.7 in 2003 • 8.5% in 2007 • 6.2% in 2011 in adults • Source UNAIDS
UM’s contribution to HIV/AIDS • Heterosexual transmission of HIV • Mother to child transmission – incl breast milk • STI’s as significant risk factors • Directed interventions prevent new infections • Male circumcision clinical trial showed protection • HIV resistance
Majengo Clinic • Focus • The health of commercial sex workers • Provides • Primary health care • Trained physicians, nurses, pharmacist • STI treatment • HIV prevention education • Condoms (male and female) • HIV counseling • HIV treatment • Research
Majengo Clinic Staff Photos by Rich Lester & Keith Fowke
Majengo Clinic Baraza 2009 Photos by Rich Lester
Nairobi Sex Worker StudyPumwani cohort • Est. in 1985, open cohort > 4000 women enrolled • Average 4 clients/day • most are HIV+ at entry, those not seroconvert within 2 yrs • ~110 uninfected despite up to 500 unprotected exposures • Exposure or co-factor determinants not different • HIV resistance defined as: • No evidence of HIV infection • Still active in sex work • Followed in cohort for >7 years
HIV Resistance – Data Summary • Resistance is not: • Absolute • Differing sexual practices • Seronegative infection • Decreased susceptibility to other infections • Coreceptor polymorphisms • enhanced b-chemokine production • Resistance associates with: • HIV-specific cellular immunity • CTL, CD4+ T cell responses in PBMC (Fowke et al.) • Mucosal CTL responses (Kaul et al.) • Qualitatively distinct responses • strong proliferation, weak IFNg(Alimonti et al.) • Genetic basis for resistance • Familial association (Kimani) • Kindred of HIV-R more likely to remain HIV-negative (Kimani, Ball) • Polymorphisms associated with resistance, e.g. IRF-1 (Ji, Ball) • Few data linking immune and genetic associations
HIV Resistance – Data Summary Hypotheses: Resistance is mediated by immune and genetic components HIV-R women will have HIV-specific T cell responses HIV-R women will have high levels of immune activation to fight infection • Resistance is not: • Differing sexual practices • Seronegative infection • Decreased susceptibility to other infections • Coreceptor polymorphisms • enhanced b-chemokine production • Resistance is: • HIV-specific cellular immunity • CTL, CD4+ T cell responses in PBMC (Fowke et al.) • Mucosal CTL responses (Kaul et al.) • Qualitatively distinct responses • strong proliferation, weak IFNg(Alimonti et al.) • Genetic basis for resistance • Familial association (Kimani) • Kindered of HIV-R more likely to remain HIV-negative (Kimani, Ball) • Polymorphisms associated with resistance, e.g. IRF-1 (Ji, Ball) • Few data linking immune and genetic associations
p=NS p0.012 p=NS p=NS p0.001 p=0.002 Immune Environment of Resistants is Different than HIV+ Resistant
HIV-specific CD4+ T cells in HESN Fowke et al Immunology and Cell Biology, 2000
p24 peptides 10 10 10 p=0.002 8 8 8 ) 3 (X10 6 6 6 cpm cpm cpm 4 4 4 cpm 2 2 2 0 0 0 ESN HIV HIV + Nlow res res res pos pos pos neglo neglo neglo n = 6 12 1 Qualitatively Distinct Responses in RESBetter Proliferative Responses p24 peptides p24 peptides p=0.002 p=0.002 ) ) 3 3 (X10 (X10 cpm cpm ESN RES HIV HIV HIV HIV + + Nlow Nlow n = 6 12 1 n = 6 12 1 Alimonti et al JID, 2005
TCM higher in Resistants S Koesters
Assessment of T cell Function • T cell functional assays • Cytokine production • Cellular activation markers • Gene expression analysis • Purified CD4+ T cells • 9 Res, 9 High-risk negatives • Whole Blood • 23 Res, 19 Low-risk negatives • Used Affymetrix U133 Plus 2.0
Res Negs Res Neg Gene expression profiling in HIV Resistants CD4 T cells Whole Blood McLaren et al JID 2010