Download
1 / 48
500 likes | 766 Views
Refraction. Švehlíková G. Department of Ophthalmology LF UPJS v Košiciach Prednosta: prof. MUDr. Juhás T., DrSc. How the Eye Sees.

E N D
Refraction Švehlíková G. Department ofOphthalmology LF UPJS v Košiciach Prednosta: prof. MUDr. Juhás T., DrSc
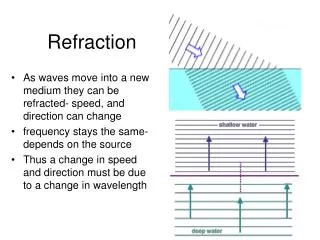
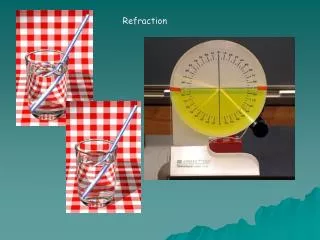
How the Eye Sees • The process of vision begins when light rays that reflect off objects and travel through the eye's optical system are refracted and focused into a point of sharp focus. • For good vision, this focus point must be on the retina, where light-sensitive cells - photoreceptors capture images in much the same way that film in a camera does when exposed to light. These images then are transmitted through the eye's optic nerveto the brain for interpretation.
refractive error • An eye that has no refractive error when viewing a distant object is said to have emmetropia or be emmetropic. • An eye that has a refractive error when viewing a distant object is said to have ametropia or be ametropic. • Very few people have refraction of exactly 0.0 diopters. • Approximately55% of persons between the ages of 20 and 30 have refraction between + 1 and–1 diopters.
refractive error • The total refractive power of an emmetropic eye is approximately 58 diopters (D), of which 43 D come from the cornea and the remaining 15 D from the lens, aqueous, and vitreous. • forms of refractive error: • Myopia (nearsightedness) • Hyperopia (farsightedness) • Astigmatism • refractive error - blurred or distorted vision
refractive error • Causes of Refractive Errors • The eye's ability to refract or focus light sharply on the retina primarily is based on three eye anatomy features: • 1) the overall length of the eye • 2) the curvature of the cornea and • 3) the curvature of the lens inside the eye
Eye Length: • If the eye is too long, light is focused before it reaches the retina, causing myopia. • If the eye is too short, light is not focused by the time it reaches the retina. This causes hyperopia.
Curvature of the Cornea: • If the cornea is not perfectly spherical, then the image is refracted or focused irregularly to create a condition called astigmatism. • A person can havemyopiaor hyperopia with or without astigmatism.
Curvature of the Lens: • If the lens is too steeply curved in relation to the length of the eye and the curvature of the cornea, this causes myopia. • If the lens is too flat, the result is hyperopia.
myopia • Raysoflightenteringtheeyefocus in front oftheretina • Therefractivepoweroftheeyeistoostrongforthelenghtoftheglobe – refractivemyopia • Theeyeistoolongfortherefractivepower – axialmyopia • Epidemiology: Approximately 25% of persons between the ages of 20 and 30have refraction less than –1 diopters.
myopia • Forms: • Simple myopia: Onset is at the age of 10–12 years • Usually does not progress after the age of 20 • Refraction rarelyexceeds 6 diopters • Pathologic ( progressive, malignant )myopia: • This disorder is largely hereditary and progresses continuously • Overgrowthoftheposterior 2/3 oftheglobe • Degenerationattheretinalperiphery • Special forms: Lenticularmyopia - sclerosis of the nucleus of the lens (cataract) in advanced age ( Spherophakia (spherically shaped lens). • Treatment:minus or concavelenses
hyperopia • Raysoflightenteringtheeyefocusbehindtheretina • Therefractivepoweroftheeyeistooweekforthelenghtoftheglobe – refractivehyperopia • Theeyeistooshortfortherefractivepower – axialhyperopia • Epidemiology: Approximately 20% of persons between the ages of 20 and 30 • have refraction exceeding +1 diopters
hyperopia • Symptoms: • In young patients, accommodation can compensate for slight tomoderate hyperopia. • However, this leads to chronic overuse of the ciliarymuscle. Reading in particular can cause asthenopic symptoms – eyepain or headache, blurred vision, ... • As accommodation decreases with advancing age, near visionbecomes difficult. For this reason, hyperopic persons tend tobecome presbyopic early. • Special forms of hyperopia: • Absence of the lens (aphakia) due to dislocation. • Postoperative aphakia following cataract surgerywithout placement of anintraocular lens • Treatment: plus or convex lenses
astigmatism • Astigmatism is derived from the Greek word stigma (point) and literally meanslack of a focal point. • parallel light rays do not focusat apoint • Therefractingpower in oneaxisisnotthesamethanthatinanaxisperpendicular to it • Epidemiology: • 42% of all humans have astigmatism greaterthan or equal to 0.5 diopters. • In approximately 20%, this astigmatism isgreater than 1 diopter and requires optical correction
astigmatism • Classification • Simplemyopicastigmatism– thefocusofonemeridianis on theretina, otheris in front oftheretina • Simplehyperopicastigmatism- thefocusofonemeridianis on theretina, otherisbehindtheretina • compoundmyopicastigmatism– bothmeridians are focused in front oftheretina • compoundhyperopicastigmatism- bothmeridians are focusedbehindtheretina • mixedastigmatism– oneisfocused in front and theotherbehindtheretina • Regular - only two meridians approximatelyperpendicular to each other • Irregular - there are multiple focal points • Causes • corneal ulcerations withresulting scarring of the cornea • penetrating corneal trauma • advancedkeratoconus • Cataract • Treatment:Cylinder lenses • Only regular astigmatism can be corrected with eyeglasses • irregular astigmatismcannot be corrected with eyeglasses
Accomodation • Abilityoftheeye to bringretinalimagesofobjects in variousdistancesintosharpfocus • Varyingthereftactivepowerofthelens • Lensisfixatedwithelasticligaments – thezonules – attheciliarymuscle. • Withcontractionofciliarymuscle, thezonulesrelaxes and thelenstakessphericalshape
presbyopia • The elasticityof the lens decreases with increasing age, and the range of accommodationdecreases • Presbyopia- physiologic loss of accommodationin advancing age - begins when the range of accommodation falls below3 diopters. • depending on agepresbyopia can be compensated withconverging lenses of 0.5–3 diopters
Anisometropia • difference in refractive power between the twoeyes • Where thedifference in refraction is greater than or equal to 4 diopters, the size differenceof the two retinal images becomes too great for the brain to fuse the twoimages into one • aniseikonia • Epidemiology: • Anisometropia of at least 4 diopters is present in less than 1%of the population • Symptoms: • Anisometropia is usually congenital and often asymptomatic. • binocular functions may remain underdeveloped • when the correction of the anisometropia results in unacceptableaniseikonia, patients will report unpleasant visual sensations ofdouble vision
Correction of Refractive Errors • the type and degree of refractive error – computerized automated refractometry • glasses, • contact lenses, • refractive surgery
Eyeglass Lenses • Monofocal • Spherical lenses • Toric lenses (cylindrical lenses) refract light only along one axis. • Spherical and toric lenses can be combined where indicated • Multifocal • different areas of the lenshave different refractive powers • Bifocals: The upper portion of the lens is for the distancecorrection; the lower portion is for the near-field correction • Patients are able to view distant objects and readusing one pair of eyeglasses • Progressive addition lenses:continuously increasing refractivepower
contact lenses • quality of the optical imageviewed through contact lenses is higher than that viewed through eyeglasses • Contact lenses have significantly less influence on the size of the retinalimage • The cornea requires oxygen from the precorneal tear film. • To ensure thissupply, contact lens materials must be oxygen-permeable. This becomes all themore important • the contact lens moves and permits circulation oftear fluid. • Contact lenses may be manufactured from rigid or flexible materials.
Rigid Contact Lenses • These contact lenses have a stable, nearly unchanging shape. • Patients takesome time to become used to them • Today, highly oxygen-permeable materials such as silicone copolymers are available • correct keratoconus
Soft Contact Lenses • The material of the contact lens, such as hydrogelis soft • Patientsfind these lenses significantly more comfortable. • The oxygen permeability ofthe material depends on itswater content, which may range from36% to 85% • Supportedby the limbus • The lens is displaced only a few tenths of a millimeterwhen the patient blinks. This greatly reduces the circulation of tear filmunder the lenses. • This requires to be removed at night to allow regenerationof the cornea
contact lenses • Contact lenses may also be classified by wearing schedule: - dailywear contacts must be removed, cleaned and stored each night, - while extended wear contact lenses are made from materials which are safe for overnight wear - sometimes "continuous wear" is used for a type of extended wear lens that can be worn for up to 30 days
Contacts can also be described by replacement interval • Daily, weekly, bi-weekly, monthly or quarterly
Special Lenses • Therapeutic contact lenses: In the presence of corneal erosion, soft contact lenses act as a bandage and thereby accelerate reepithelializationof the cornea. They also reduce pain.
Disadvantages of Contact Lenses • Contact lenses exert mechanical and metabolic influences on the cornea. • Therefore, they require the constant supervision of an ophthalmologist. • Contact lenses require carefuldaily cleaning and disinfection. • This is more difficult, time-consuming, andmore expensive than eyeglass care
Contact Lens Complications • Infectious keratitis (corneal infiltrations and ulcers) caused by bacteria,fungi, and protozoans • Giant papillary conjunctivitis: This is an allergic reaction of the palpebralconjunctiva of the upper eyelid • Corneal vascularization may be interpreted as the result of insufficientsupply of oxygen to the cornea • Severe chronic conjunctivitis: This usually makes it impossible to continuewearing contact lenses
refractive surgery • is surgical (laser or conventional) configuring of the curvatures of the eye (cornea and/or lens) to allow the rays of light to be focused on the retina as a point • Categories • Cornealrefractive procedures • Intraocularrefractive procedures
refractive surgery Cornealrefractiveprocedures Intraocularrefractive procedures
refractive surgery • lower refractive errors (in the range +4.00 to -10.00D) are usually corrected using laser techniques to reshape the cornea • higher errors are corrected using lens implant based methods • astigmatism and age are also influential in determining the most appropriate technique
Laser Refractivesurgery • an eye drop anesthetic is used • A portion of the cornea is removed, or creatingtheflap • The eye is then positioned under an Excimer laser which has been programmed to remove microscopic amounts of corneal tissue. • Removal of the tissue changes the curvature of the cornea. • If the patient has myopiatissue closer to the central part of the cornea is removed to decrease the curvature or flatten the cornea. • If a patient has hyperopiatissue in the periphery of the cornea is removed to increase curvature. • To correct for astigmatism, selected tissue at certain angles is removed to insure that the cornea curves equally in all directions. • After the laser has been used, the flap is returned to its original position.
Laser Refractivesurgery Profile ofthecorneaafterfotoablationfor MYOPIA Profile ofthecorneaafterfotoablationfor HYPEROPIA If the patient has myopiatissue closer to the central part of the cornea is removed to decrease the curvature - flatten the cornea If a patient has hyperopia tissue in the periphery of the cornea is removed to increase curvature
Laser Refractivesurgery • dividedinto • lamellar (LASIK) and • surface ( PRK, LASEK, and Epi-LASIK) • laser-assisted in situ keratomileusis(LASIK) • photorefractive keratectomy (PRK) • laser assisted subepithelial keratectomy (LASEK)
PRK, LASEK, and Epi-LASIK • methods of surface ablation • these procedures do not require a partial thickness cut into the stroma • these methods differ in the way the epithelial layer is handled
photorefractive keratectomy (PRK) • In photorefractive keratectomy surgery the epithelium is removed • The epithelium might be removed in several ways, including excimer laser destruction, mechanical debridement with a surgical blade, abrasion with a brush, or use of alcohol to loosen the epithelium.
Laser assisted subepithelial keratectomy (LASEK) • LASEK – epitelialflap • Epi-LASIK - microkeratome • In LASEK and Epi-LASIK surgery the epithelial flapis foldedback • after the ablation, this epithelial flapis placed back into its original position • the epithelial alignment is protected from blinks and eye movements by the addition of a bandage contact lens
LASEK The Advantages The Disadvantages • No stromal flap - much fewer serious potential complications ( Lamellar Keratopathy, Interface infections.) • Minimal or no induction of optical aberrations • Quicker recovery of corneal sensation and the blink reflex (4 months vs. 1 1/2 years with LASIK) • Higher amounts of refractiveerrorscan be corrected • More discomfort • Recovery time is longer • final results for LASIK and surface treatments are similar
laser-assisted in situ keratomileusis(LASIK) • a partial-thickness corneal flap • made with a microkeratome • depths of 100–200 µm • femtosecond laser has been developed, provides more accuracy in flap thickness
LASIK The Advantages The Disadvantages • Rapid visual recovery • Less postoperative discomfort • Induces more optical aberrations • Induces more complications • If there is a complication, it is usually due to the flap • Only used for mild to moderate myopia • Much longer time for recovery of blink reflex when the eye is dry
Complications • Corneal scarring/haze (<1-2%) • Although LASEK may carry a decreased rate of corneal haze relative to PRK, it may still develop secondary to an inflammatory response to the surgical manipulation of the corneal surface. • The inflammation leads to the formation of an opacified cellular layer that appears as a white haze and restricts light from transmitting to the back of the eye, thus causing a defect in vision • The risk of scar formation increases with increasing ablation depth, and scars are common when treating more than 8 D of myopia. • Keratitis (0.5-1%) • Postoperative infection is more likely when epithelial coverage is incomplete or when the surgical duration is longer than average. • Additionally, contact lenses may serve as a source of infection, as they may be contaminated with microorganisms. Likely, because contact lenses are not used postoperatively in LASIK, LASIK has a lower incidence of keratitis (about 0.2%).
Complications Corneal scarring/haze Keratitis
Complications • Dry eye syndrome associated with recurrent erosions • This complication is secondary to decreased corneal sensation due to corneal denervation. It may last from a few weeks to 1 year, although, on average, it lasts 1-4 weeks. • Although this complication occur in LASEK and LASIK, it is more likely to be associated with a longer duration in LASIK. • Overcorrection (1%, incidence similar to LASIK and PRK) • Undercorrection (10-15%, incidence similar to LASIK and PRK) • Macular cyst formation (<0.1%) • Irregular astigmatism (<1%): This complication is secondary to decentration of the laser optical zone or uneven healing, leading typically to a wavy corneal surface.
Intraocularrefractive procedures • Clearlensextraction • range:myopia/hypermetropia atany level • Principle = replacement of the natural lens with an intraocular lens (IOL) • multifocal IOLs can be implanted to reduce spectacle dependence for near vision • is identical to modern cataract surgery
Intraocularrefractive procedures • Phacicintraocularlens • implantation - range: up to -17D myopia; up to +10D hypermetropia • Principle = implantation of a soft flexible artificial lens • is particularly suited to younger patients who are out of range for laser refractive surgery
Indications • The major indications for refractive surgery include astigmatism, myopia, and hyperopia, specifically in patients who are intolerant of or who desire to be free from glasses or contact lenses
Contraindications • Unstable refractive error • Refractive error outside the range of correction (The range varies according to the surgeon's experience, the laser used, and the laser strategy; however, it is typically approximately 9-14 D of myopia, 4-6 D of hyperopia, and 2-6 D of astigmatism.) • Keratoconus • Pellucid marginal degeneration • Significant dry eye syndrome • Active inflammation of external eye • Autoimmune disease • History of or active herpes simplex keratitis, risc of the reactivation of the virus • Active collagen vascular disease • Uncontrolled diabetes • Uncontrolled glaucoma • Pregnancy or breastfeeding