Download
1 / 31
320 likes | 344 Views
Stay updated on the HSCRC's regulatory requirements for hospital revenue compliance and market shift adjustments. Learn about the Global Budget/Total Patient Revenue (GBR/TPR) compliance guidelines, penalties for non-compliance, unit rate adjustments, and moving services from regulated to unregulated settings. Gain insights into the FY 2016 Market Shift Adjustment, including factors considered and financial impacts. Stay informed to ensure your hospital maintains compliance with the latest regulations.

E N D
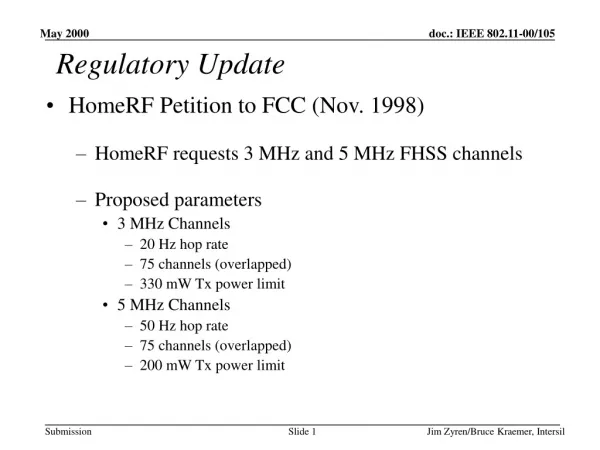
HSCRC Regulatory Update Mitch Lomax, Saint Agnes Healthcare Jerry Schmith, Maryland Health Services Cost Review Commission August 21, 2015
GBR/TPR Compliance • Two sets of Price Corridors for GBR and TPR hospitals: 1). Overall Approved Total Revenue Levels under GBR or TPR agreement. 2). Unit Rate Compliance • Referencing Documents: 1). October 2014 Addendum to Global Budget Agreement – Section V. Compliance 2). October 6, 2014 HSCRC memo “December 31, 2014 Revenue Targets and Unit Rate Compliance” 3). March 20, 2015 HSCRC memo “Unit Rate Compliance”
GBR/TPR Compliance • Interim (6-month) GBR/TPR compliance • Target equal to 50% of overall GBR/TPR target for most hospitals (hospitals with significant seasonality may have a different target) • Target provided to assure that statewide revenue for the calendar year does not exceed the revenue limits provided under the new waiver agreements • Hospitals expected to maintain charges at or below this limit. • “Soft target” for CY 2014 - No penalties applied for not complying with CY 2014 interim targets. • Unit rate compliance penalties were not applied at December 31, 2014
GBR/TPR Compliance • Annual GBR/TPR Compliance • Hospitals are expected to monitor and adjust unit rate charges on an ongoing basis to ensure that it operates within the Annual GBR target. • Price Variances will be added/subtracted to the GBR target for the subsequent rate year. • To assure compliance, HSCRC staff will apply penalties for charges outside of the overall GBR/TPR revenue target: * If HSCRC staff determines that a hospital intentionally overcharged, then the overcharge corridor exempting an overcharge of up to 0.5% will be eliminated, and a 20% penalty will be applied.
Unit Rate Compliance • Hospitals may increase or decrease rates across all rate centers within a +/- 5% corridor without notifying the Commission. • If hospitals need to increase or decrease rates by more than 5% to maintain overall GBR compliance, it must notify the Commission staff. • Limit may be extended to +/-10% at the discretion of the HSCRC staff, provided the hospital provides satisfactory evidence (including documentation) that this expansion is necessary to meet the revenue constraints for the Rate Year. • All approved requests will be granted for a maximum of three months. Hospitals are free to submit requests to continue these approvals.
Unit Rate Compliance • Hospitals will generally need to spread rate adjustments across all centers, avoiding adjustments concentrated in a few rate centers, unless it has received approval from the HSCRC staff for an alternative approach. • Unit rate compliance will be measured for the full rate year. However, compliance is measured by staff monthly, and any large rate shifts among centers will be addressed. • Interim penalties for three consecutive months (rolling compliance) are not imposed • Charges beyond corridor shall be subject to penalties (40% of price variance).
Unit Rate Volumes in Rate Order Compares price-leveled volume for 12 months ended March 2015 to FY 14 rate order volume.
Unit Rate Volumes in Rate Order Aggregate volume change is applied across the board to all rate centers.
Unit Rate Volumes in Rate Order Demographic, market shift and MA utilization adjustments are applied to these adjusted volumes.
Moving Services from Regulated to Unregulated • The GBR/TPR agreement requires a hospital to notify HSCRC staff if it moves services from an HSCRC regulated setting to an unregulated setting • Once notified, hospital and HSCRC staff may negotiate a GBR/TPR cap adjustment to reflect the service shift • Considerations can include: • Market impact • Fixed/variable costs • Replacement services • Impact on Medicare spend
HSCRC Market Shift • Rate Year 2016 rate orders reflect the HSCRC’s market shift adjustment, developed during the Fall 2014 / Spring 2015 • In summary: • Algorithm determines the “shift” among hospital volumes in each market (zip code + service line; certain counties were aggregated from all county zip codes) • Volume increases compared to volume decreases • The smaller utilization change, increase or decrease, becomes the market limit • See the example on the next page • Excludes potentially avoidable volume • Volumes are measured using Equivalent Case Mix Adjusted Discharges (ECMAD) • Financial impacts are calculated on a hospital and service line specific charge per ECMAD • HSCRC released its “final” RY2016 calculation on July 8, excluding outpatient oncology. The results are reflected on page 15.
HSCRC Market Shift • Market Shift example (HSCRC, Payment Models Work Group, January 12, 2015)
HSCRC Market Shift • In the July release, outpatient oncology services – infusion, chemotherapy and radiation therapy - were excluded as a result of “cycle” versus “individual” billing. • Individual patient records, and therefore EAPG weights, were not comparable among hospitals. • To address this, HSCRC staff developed an alternative case weighting method for outpatient oncology services (draft results on the next page) • Aggregates patient records using CRISP EID (or hospital medical record numbers if EID isn’t available) • Assigns an EAPG hierarchy: infusion, chemotherapy and radiation therapy • Calculates an average “per diem” charge, dividing charges by patient “length of stay” based on “From” and “Thru” dates • To create an outpatient weight, the average EAPG per diem charge is divided by the average outpatient charge per visit • The average weight is multiplied by each hospital’s “length of stay” to calculate the total outpatient case weight
Rate Year 2016 Demographic Adjustment • The HSCRC’s demographic adjustment is applied to annually to hospital rates. • Essentially a “prospective” adjustment for volume and service mix change • The demographic adjustment reflects: • Age weighted population growth • Adjustment for potentially avoidable utilization • Each hospital’s unique service market (based on ECMAD) • The aggregate results are then adjusted to the statewide average population growth reflected in the annual update, with certain adjustments
FY 16 Uncompensated Care Policy • Establishes Uncompensated Care Funded in Hospital Rates • 50% based on 2-year actual UCC per hospitals audited financials • 50% based on a predicted amount as determined by a regression • For FY 16, UCC in rates was “frozen” at FY 15 amounts • January 1, 2014, ACA expansion occurred which significantly expanded Medicaid coverage • Data reporting lag of UCC policy made it near impossible to reflect recent increase in Medicaid population • The mid-year Medicaid expansion does not line up with the historical July – June measurement period of the UCC policy. • Reporting challenges exist as it relates to hospitals reporting of the Medicaid Pending population
FY 16 Uncompensated Care Policy • Since UCC policy was frozen, the HSCRC prospectively reduced UCC provisions to reflect the January 1, 2014 Medicaid expansion. • FY 15 • Prospective reduction limited to conversion of the Primary Adult Care (PAC) program to Medicaid. • Did not include anticipated reductions as a result of MA expansion (116% - 138% FPL) • Result 1.09% statewide reduction • FY 16 • Used Medicaid enrollment file along with HSCRC data (using MPI) to analyze reduction in self pay and increase in Medicaid charges. • Approach effectively captured remaining MA expansion population • Result 0.89% statewide reduction Total 2-year statewide reduction 1.98%
FY 16 Uncompensated Care Policy • Prospective reduction for Medicaid expansion should be included in the Medicaid portion of the Payer Differential calculation of hospitals rate order to account for the 6% discount provided to Medicaid payers.
FY 16 Uncompensated Care Policy • Medicaid expansion also resulted in an increase in the utilization of hospital services for newly eligible Medicaid beneficiaries. • Reflects pent up demand thought to be largely temporary (e.g. orthopedics/surgery) • Temporary growth funded in FY 15 by excess UCC in rates • Permanent portion of this utilization growth was built into hospitals Global Budget Revenue targets for FY 16. • Permanent portion of growth was based on growth rate for Quarter 4 of 2014 of 21% (50% variable cost factor applied). • Results in $57.4 million in additional statewide funding.
FY 17 UCC Policy Considerations • UCC Policy will likely need a major redesign since the landscape has changed with ACA insurance expansion. • Medicaid coverage as a predictive variable may no longer be appropriate • Undocumented population continues to be a highly uninsured population • More high deductible plans offered on the insurance market meaning more after insurance uncompensated care • Potential change could be looking at poverty rates of hospitals service area. • Is there a high correlation between zip codes’ rate of poverty and the likelihood of a patient from that zip code resulting in UCC?
CMS Payment Bundle • On July 14, CMS released its Comprehensive Care for Joint Replacement (CCJR) proposed payment rule • Hospitals at risk for episodes of care, including physician, SNF and other services, versus an established target • All providers are paid on a fee-for-service basis, less some savings, with the hospital settling the overall difference versus the target • Hospitals are responsible but can share risk with collaborating providers • Waives certain policies (receive a certain number of home health visits without qualification, allows telehealth and waives 3-day rule beginning in year 2) • CMS invited Maryland to comment in the context of our new Waiver
CMS Payment Bundle • Coordination of care is critical to Maryland All-Payer model and tools provided under this model could assist Maryland in achieving cost targets. • Given Maryland’s all payer nature, existing incentives and increasing focus on total cost of care, implementation may take a different path. • E.g., Maryland hospitals cannot be paid under normal Medicare DRG payment rates • The data and tools under the CCJR model are needed to successfully align initiatives in Maryland. • HSCRC staff plan to: • Work with stakeholders to craft a comment and request data to evaluate opportunities • Ask for access to the same tools, while considering the opportunity in the broader context of health improvement