Download
1 / 52
520 likes | 675 Views
Practical Genetics for Primary Care. 6 th February 2013 Kate Carter Genetic Counsellor Nottingham Clinical Genetics Service Telephone: 0115 962 7728 Email: nuhnt.clinicalgenetics@nhs.net. Overview. Introduction to genetics for GPs Taking a family history Family cancer genetics

E N D
Practical Genetics for Primary Care 6th February 2013 Kate Carter Genetic Counsellor Nottingham Clinical Genetics Service Telephone: 0115 962 7728 Email: nuhnt.clinicalgenetics@nhs.net Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Overview • Introduction to genetics for GPs • Taking a family history • Family cancer genetics • Making a referral to the genetic department • Sources of further information • Ethical dilemmas Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Identifying patients Communicating genetic information Clinical management When might a GP see genetics in practice? Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Common / important conditions Autosomal recessive disorders Cystic Fibrosis Haemoglobinopathies Haemochromatosis X-Linked disorders Duchenne and Becker Muscular dystrophies Haemophilia A Fragile X Variable inheritance patterns Deafness Muscular dystrophies Chromosomal disorders Syndromes: Down, Turner, Klinefelter. Chromosomal Translocations Autosomal dominant disorders Adult polycystic kidney disease Neurofibromatosis Huntington Disease Hypercholesterolemia Marfan Syndrome Familial Cancer Bowel/Uterine/Ovarian ?HNPCC Breast/Ovarian/Prostate ?BRCA1/2 Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Questions a patient may ask • What’s wrong? • What does the future hold? • Is there a cure? • Why did it happen? • Will it happen again? • Will it be as bad or worse? • Whose fault is it? • Are there any tests? • Who else is at risk? Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Why is the patient asking their question now? Recent diagnosis? Anniversary of a birth/death of an affected family member? Approaching the age others became affected? Screening becoming available? Planning marriage/beginning a family/buying a house? Pressure from family/friends? Religious aspects? Media reports about the condition? Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Is my baby at risk of cystic fibrosis? Supporting Genetics Education for Health www.geneticseducation.nhs.uk
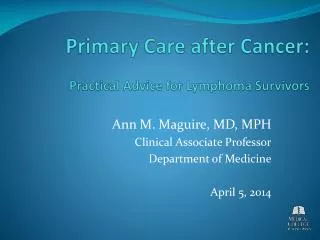
Scenario… • Watch a video of a GP being consulted by Jane Hobson. She is in the early stages of pregnancy and is consulting him about the risks to her baby of having cystic fibrosis. Her nephew, Richard Whitehead, was diagnosed as having cystic fibrosis as a result of the neonatal cystic fibrosis screening programme. • The medical family tree (pedigree) will be taken from Jane Hobson. Please draw out the pedigree as it is being taken. Supporting Genetics Education for Health www.geneticseducation.nhs.uk
/ P X weeks Pedigree Symbols Male Marriage / Partnership (horizontal line) Female Partnership that has ended Person whose sex is unknown Offspring (vertical line) Pregnancy Miscarriage Parents and Siblings Affected Male & Female Carrier Male & Female Supporting Genetics Education for Health www.geneticseducation.nhs.uk
CF video family history clip Supporting Genetics Education for Health www.geneticseducation.nhs.uk
William Joan George Joan 60 63 63 Died age 65, 2007 Christopher Hobson Jane Julie John Whitehead Christine 29 29 27 27 30 P 9 weeks 6 weeks David Richard 10 Born 2004 Cystic fibrosis Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Joan William Joan 63 George Whitehead 63 60 Died age 65, 2007 Christopher Hobson Jane Julie John Whitehead Christine 29 29 27 27 30 P 9 weeks 6 weeks David 10 Richard Born 2004 Cystic fibrosis From the family pattern, who must be carriers for cystic fibrosis? Supporting Genetics Education for Health www.geneticseducation.nhs.uk
William Joan George Joan 60 63 63 Died age 65, 2007 Christopher Hobson Jane Julie John Whitehead Christine 29 29 27 27 30 or P 9 weeks 6 weeks David Richard 10 Born 2004 Cystic fibrosis Is the probability of Jane Hobson being a carrier for cystic fibrosis sufficiently high to offer testing? Supporting Genetics Education for Health www.geneticseducation.nhs.uk
William Joan George Joan 60 63 63 Died age 65, 2007 Christopher Hobson Jane Julie John Whitehead Christine 29 29 27 27 30 P 9 weeks 6 weeks David Richard 10 Born 2004 Cystic fibrosis Assume Jane was tested and found to be a carrier. What is the probability that the baby in Jane and Christopher Hobson’s current pregnancy will have cystic fibrosis? Supporting Genetics Education for Health www.geneticseducation.nhs.uk
William Joan George Joan 60 63 63 Died age 65, 2007 Christopher Hobson Jane Julie John Whitehead Christine 29 29 27 27 30 P 9 weeks 6 weeks David Richard 10 Born 2004 Cystic fibrosis At what stage should specialist genetic advice be sought? Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Genetic family history • 1. Why is family history information important to my practice? • 2. How do I collect and record family history information? • Factsheets, animations, slides and videos • ‘Medical Family History Drawing Tool’ • Worksheets for practising drawing pedigrees • 3. How do I interpret family history information? • Factsheets and slides on ‘Understanding Modes of Inheritance’’ • Factsheets and worksheets on ‘Interpreting a Family History’ Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Familial Cancer Genetics • When to make a referral • Who to refer to • Sources of information and advice Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Dominant breast cancer genes • BRCA1 and BRCA2 identified. Possibly BRCA3 and others? • Lifetime risk of breast cancer 50 - 85% • Carry risk of other cancers; ovary (BRCA1 44%, BRCA2 27%), and a slightly increased risk prostate and some other cancers Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Autosomal Dominant Inheritance Parents Gametes At conception Unaffected Affected
Hereditarygene change 1 Somatic mutation Somatic mutation Cancer Normal Tissue
Hereditarygene change Somatic mutation 2 Somatic mutations Cancer Cancer
What factors do you think may indicate a woman is at higher risk of breast / ovarian cancer? Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Case 1 • Low risk – manage in primary care • Older age of onset • Different sides of the family 65 Breast cancer 70 76 46 Kay 51 49 55 53 Reassure and explain population risk, advise on symptom awareness and to report any changes in family history
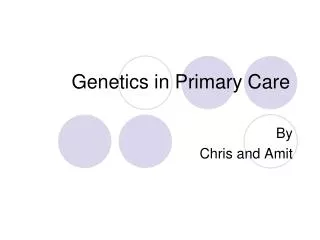
Case 2 • Refer –high risk • Different generations • Young age onset • Equal transmission through men • Multiple tumours in one individual • Breast and ovarian cancer 42 48 breast cancer 56 ovarian cancer Breast cancer Ovarian cancer 32 Janet 35 Refer – to Wendy Chorley (familial cancer service) – Royal Derby Hospital. They will offer a referral to genetics where indicated.
Familial Colorectal Cancer • Colorectal cancer common – 1 in 25 • 5-10% strong genetic contribution • The most important of these genetic syndromes are: - familial adenomatous polyposis(FAP) - Lynch Syndrome, or hereditary non-polyposis colorectal cancer (HNPCC) • Most dominant – not all! Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Case 3 • Refer –moderate risk • Young age of onset (under 45) 35 died in war 68 73 60s 77 78 43 73 75 32 Peter Colorectal cancer Refer to Wendy Chorley Familial Cancer Service Royal Derby Hospital - first degree relatives offered bowel screening. No genetic testing available
Case 4 • Refer –high risk • Young age of onset • Endometrial and bowel cancers (other related cancers include ovarian, ureteric, renal pelvis, gastric) • Two generations • Polyps 55 49 69 42 George 80 75 48 78 Endometrial cancer 39 Polyps 30 Martin 42 Colorectal cancer Refer to Wendy Chorley - diagnoses would be confirmed, offer genetic testing to George. Bowel screening would be offered to at-risk family members.
Assessing cancer risk • Young age of onset, pattern of similar tumours in a family (or multiple primaries in one person) • Related tumours • Remember ethnicity e.g. Chinese, Indian, Ashkenazi Jewish ancestry • Use national / local guidelines e.g. NICE familial breast cancer • Over 200 hereditary cancer syndromes described – individually rare • Contact the CGS if you are unsure Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Making a referral to clinical genetics • Information needed • Patient’s name, D.O.B, address, GP • date of last period or due date (if pregnant) • Details of concern, name of affected person and D.O.B if possible and how they are related to your patient. • Patient’s telephone number – home and daytime contact Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Making a referral to clinical genetics • Most referrals can be sent by post or C&B • Urgent referrals should be made by telephone • A referral is urgent if • The patient is pregnant • The patient is in the last stages of a terminal illness Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Sources of information • Local or national guidelines e.g NICE • Discussing with a colleague • Contact the local CGS • Internet Supporting Genetics Education for Health www.geneticseducation.nhs.uk
National Genetics Education and Development Centre Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Supporting Genetics Education for Health www.geneticseducation.nhs.uk
To refer or not refer? • Please call Nottingham Regional Clinical Genetics Service for advice and information • Tel: 0115 962 7728 Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Referral Address Nottingham Clinical Genetics Service, City Hospital Campus, The Gables, Gate 3, Hucknall Road Nottingham NG5 1PB Tel: 0115 962 7728 Fax: 0115 962 8042 Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Ethical Issues in Primary Care Genetics Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Mr P has been diagnosed with long QT syndrome (a heart condition which can result in sudden death). This is a dominant condition, so his 4 children (aged from 10-19 years) are all at 50% risk. Testing is advised in childhood, as there are health and screening implications for affected family members. Mr P tells you in confidence that one of his children is adopted (and therefore not at genetic risk) but does not know this. How might we proceed? Supporting Genetics Education for Health www.geneticseducation.nhs.uk
A similar situation… Cystic fibrosis A couple have a newborn child who is diagnosed with cystic fibrosis. As a routine next step, we counsel them about having carrier testing to confirm their carrier statuses, as this allows testing in future pregnancies and allows carrier testing for the wider family. The wife calls after the clinic to confess that she is uncertain whether her husband is the father of her baby, and does not want us to test him, for fear of disclosure. Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Duchenne muscular dystrophy (DMD) is a progressive neuromuscular disorder affecting approximately 1 in 3000 male births. Boys with DMD are usually diagnosed between 4-5 years of age. In about two thirds of cases, the boy’s mother is a carrier for the condition, and at risk of having another affected boy. There is no cure for DMD. Neonatal screening of all male births should be performed to identify affected boys so that their mothers can be tested to see if they are a carrier and therefore at risk of having further affected children. Consider the statement above and indicate the extent to which you agree or disagree with it. Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Strong family history of breast / ovarian cancer (BRCA1) No knowledge Eve, BRCA1 Erica, 35 Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Erica is 35 and registers as a new patient at her GP surgery. When registering, Erica is asked if she has any family history of concern, and states that she does not. Erica's paternal aunt Eve is also registered with the GP practice, but the two branches of the family have no contact. The GP recognises their unusual surname and remembers speaking with Eve about her strong family history of breast cancer. Upon checking his records, the GP realises that Erica will be at risk of carrying the BRCA1 genetic change in the family. The GP has an obligation to tell Erica, his new patient, information which he knows may affect her health and access to screening in the future. Consider the statement above and indicate the extent to which you agree or disagree with it. Supporting Genetics Education for Health www.geneticseducation.nhs.uk
A consanguineous couple attend the genetics clinic as they have a 7 year old son affected by Duchenne Muscular Dystrophy (DMD). They are pregnant again and request prenatal testing. Fetal sexing is first offered and shows the baby to be female. Female carriers of DMD are healthy, and do not have muscle problems. This couple still request a CVS (with an associated 1% risk of miscarriage) to determine if the baby is a carrier. They say they will end the pregnancy if this child is a carrier. What should you do? Test Uncertain Not test Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Jane is a healthy, 24 year old patient. She comes to speak to you about her family history of Huntington Disease (HD, an autosomal dominant condition), explaining that her maternal grandmother was affected and died 1 year ago, in her 60s. Jane is aware that genetic testing is available to her family, and Jane wishes to request this, to determine if she will develop the condition herself in the future. You ask Jane how her mother feels about this issue, and Jane tells you that her mother has declined genetic testing. If Jane is tested and shown to have an expansion which causes HD, you will also have clarified that her mother will develop HD. Jane should not be offered genetic testing without first testing her mother. Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Cystic fibrosis Homozygous for very rare genetic change Supporting Genetics Education for Health www.geneticseducation.nhs.uk
Jo Dan P 8 years Cystic fibrosis 4 years Supporting Genetics Education for Health www.geneticseducation.nhs.uk