Download
1 / 1
10 likes | 491 Views
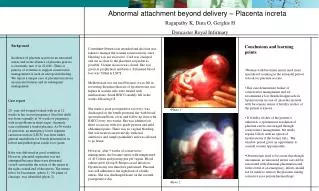
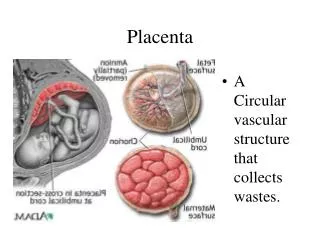
Placenta accreta is an abnormal invasion of the placenta into the myometrium . The incidence of placenta accreta has dramatically increased due to increasing caesarean section rate. Placenta praevia major with accreta is associated with significant maternal morbidity and mortality.

E N D
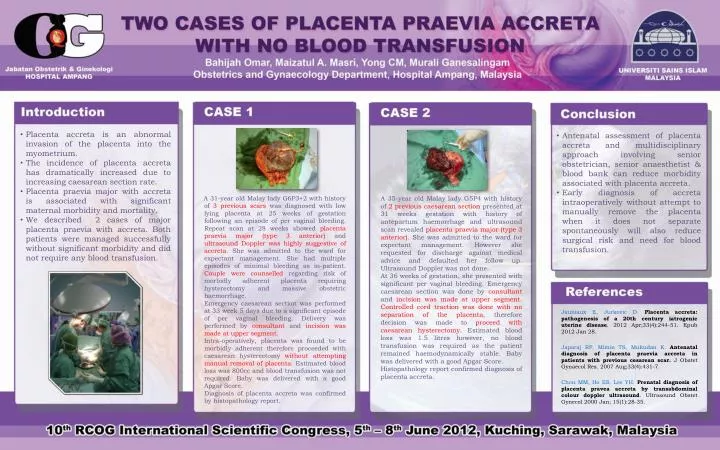
Placenta accreta is an abnormal invasion of the placenta into the myometrium. • The incidence of placenta accreta has dramatically increased due to increasing caesarean section rate. • Placenta praevia major with accreta is associated with significant maternal morbidity and mortality. • We described 2 cases of major placenta praevia with accreta. Both patients were managed successfully without significant morbidity and did not require any blood transfusion. • Antenatal assessment of placenta accreta and multidisciplinary approach involving senior obstetrician, senior anaesthetist & blood bank can reduce morbidity associated with placenta accreta. • Early diagnosis of accretaintraoperatively without attempt to manually remove the placenta when it does not separate spontaneously will also reduce surgical risk and need for blood transfusion. A 31-year old Malay lady G6P3+2 with history of 3 previous scars was diagnosed with low lying placenta at 25 weeks of gestation following an episode of per vaginal bleeding. Repeat scan at 28 weeks showed placenta praevia major (type 3 anterior) and ultrasound Doppler was highly suggestive of accreta. She was admitted to the ward for expectant management. She had multiple episodes of minimal bleeding as in-patient. Couple were counselled regarding risk of morbidly adherent placenta requiring hysterectomy and massive obstetric haemorrhage. Emergency caesarean section was performed at 33 week 5 days due to a significant episode of per vaginal bleeding. Delivery was performed byconsultant andincision was made at upper segment. Intra-operatively, placenta was found to be morbidly adherent therefore proceeded with caesarean hysterectomy without attempting manual removal of placenta. Estimated blood loss was 800cc and blood transfusion was not required. Baby was delivered with a good Apgar Score. Diagnosis of placenta accreta was confirmed by histopathology report. A 35-year old Malay lady G5P4 with history of 2 previous caesarean section presented at 31 weeks gestation with history of antepartum haemorrhage and ultrasound scan revealed placenta praevia major (type 3 anterior). She was admitted to the ward for expectant management. However she requested for discharge against medical advice and defaulted her follow up. Ultrasound Doppler was not done. At 36 weeks of gestation, she presented with significant per vaginal bleeding. Emergency caesarean section was done by consultant and incision was made at upper segment. Controlled cord traction was done with no separation of the placenta, therefore decision was made to proceed with caesarean hysterectomy. Estimated blood loss was 1.5 litres however, no blood transfusion was required as the patient remained haemodynamically stable. Baby was delivered with a good Apgar Score. Histopathology report confirmed diagnosis of placenta accreta. Jauniaux E, Jurkovic D. Placenta accreta: pathogenesis of a 20th century iatrogenic uterine disease.2012 Apr;33(4):244-51. Epub 2012 Jan 28. Japaraj RP, Mimin TS, Mukudan K. Antenatal diagnosis of placenta praeviaaccreta in patients with previous cesarean scar. J ObstetGynaecol Res. 2007 Aug;33(4):431-7. Chou MM, Ho ES, Lee YH. Prenatal diagnosis of placenta praveaaccreta by transabdominalcolourdoppler ultrasound. Ultrasound ObstetGynecol 2000 Jan; 15(1):28-35.