Download
1 / 40
400 likes | 593 Views
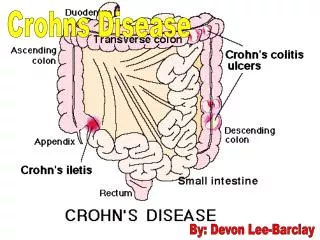
Crohn`s Disease. It is an idiopathic ,chronic ,transmural inflammatory process of the bowel ,that can affect any part of the GI tract ,most cases involve terminal ileum.It is believed to be a result of an imbalance between pro inflammatory and anti-inflammatory mediators.Unpredictable flares

E N D
1. Infliximab Maintenance Therapy for Fistulating Crohn`s Disease New England journal of Medicine
Feb. 26,2004
Directed by: Dr. A. HAMAM
Presented By:Dr.Y.Abu-Zanouna
2. Crohn`s Disease It is an idiopathic ,chronic ,transmural inflammatory process of the bowel ,that can affect any part of the GI tract ,most cases involve terminal ileum.
It is believed to be a result of an imbalance between pro inflammatory and anti-inflammatory mediators.
Unpredictable flares & remissions.
3. Pathophysiology The exact cause remains unknown
Theories: genetic microbial,immunologic, environmental, dietary, vascular ,psychosocial.
Microscopically : inflammation around the crypts, ulceration ,granuloma , mesentery & lymph nodes.
Macroscopically : Hyperemia & edema , ulcers � cobble stone � ,segmental lesions
4. Genetics 1st degree relatives have a 5-25% higher risk than normal population.
Family members of patients with Crohn`s Disease have increased risk for both CD & UC.
Offspring have an 8.9% & siblings an 8.6% risk for developing IBD
Susceptibility regions detected on different chromosomes (6 ,12 , 16 )
5. Epidemiology Incidence rate in children 3.5/100,000 in NA 10 � 19 yr olds.
More than 1/3 of patients present in childhood or adolescence.
Family history is present in 30% ,younger than 30.
Males = Females in adulthood, Males > females in childhood.
Highest incidence in Caucasians.
6. Clinical Presentation Weight loss 85%
Diarrhea 80 %
Abdominal pain 85%
Rectal bleeding 50%
Growth failure 35%
Fever 40%
Rectal disease 25%
Extraintestinal signs 25%
Perianal disease 25%
Nausea& vomiting25%
7. Clinical presentation Physical examination:
Growth Delay , wt loss , delayed puberty
RLQ mass & tenderness
Palpable thickened loop of intestine
Hyperactive bowel sounds
Perianal & rectal examination: skin tag ,fissure ,fistula, hemorrhoids or abscess.
8. Laboratory Aids Anemia:
Chronic inflammation
Malabsorption ( B 12 & folate )
Chronic blood loss
Leukocytosis:
Chronic inflammation
Abscess
Steroid treatment
9. Lab`s Hypoalbuminemia
Hypocholestrolemia
Hypocalcaemia
Hypomagnesaemia
High CRP & ESR
P-ANCA : CD 19% vs. UC 80%
ASCA : Anti � Saccharomyces Crevisiae Antibdy;
CD 60%
10. Imaging Studies Plain Abdominal radiograph
Barium contrast studies
CT scan
MRI
U/S
Radionucleotide Scans
11. Procedures Colonoscopy :
Obtaining multiple biopsies : diagnostic
Dilatation of fibrotic strictures
Upper endoscopy:
Differentiating Crohn`s from other disease
ERCP : diagnostic & therapeutic
12. Differential Diagnosis UC
Appendicitis
Infection
HUS
HSP
Irritable Bowel Syndrome
Immune deficiency
PUD
TB
Lactose intolerance
SI Lymphoma
Psychosocial disturbance
13. Complications Obstruction( 8-40 %)
Transient ; stricture formation
Fistulization:
Enteroenteral ,entervesical ,enterovaginal ,enterocutaneos
Abscess formation
Perianal Disease (25-50%)
Adhesions
Malabsorption
Growth Failure
14. Treatment Medical Care:
Diarrhea
Abdominal pain
Diet & nutritional therapy:
Balanced , high Fiber
Low fat , MCTG
Enteral therapy ,elemental diet in acute disease
TPN
15. Medical Treatment 5 � ASA preparations
Steroids
Immunosuppressants: Azathioprine , 6 MP.
Antibiotics
If medical treatment fails, surgical resection of the involved part of bowel is resected .
16. Fistulae Fistulae between Bowel loops are usually benign & may not produce major problems
Enterovesical, enterocutaneous , cologastric , coloduedenal are more serious .
Surgery : progressive obstruction,abscess, malabsorption.
Medically : Metronidazole, Ciprofloxacin
17. New Medical Therapies Immunosupressive agents : Tacrolimus
Mycophenolate mofetil
Anti inflammatory Cytokines : IL 10, IL11
18. INFLIXIMAB Monoclonal Antibody against TNF
It blocks TNF in the serum & at the cell surface, leading to lysis of TNF-producing macrophages & T-cells.
In one study ~ 65% of refractory cases of CD responded well to Rx with infliximab & 1/3 went into remission.
Patients who relapsed , responded again to further infusions.
Effective in patients with Fistulae ,median duration of response 12 wks.
19. INFLIXIMAB Before starting treatment :
Allergies : Infliximab , rodents
Pregnancy: Studies have not been conducted.
Breast Feeding:Not known whether it is excreted in breast milk or not
Medical problems:
Congestive Heart Failure
Active infections
Tuberculosis infection ( PPD)
20. Infliximab in Children?! Studies on this medicine have been done ONLY in adult patients; there is no specific information comparing use of infliximab in children with use in other age groups.
21. Side Effects Common : chest pain, fever , flushing, S.O.B , Abdominal pain, N/V , headache , fainting, muscle pain , sore throat , nasal congestion
Less common : Back pain, hematuria ,dysuria,urgency, stomatitis.
Rare:Weight loss ,thrombocytopenia
22. Other uses Ankylosing Spondylitis
Psoriasis
Reactive arthritis
Rheumatoid Arthritis
Inflammatory bowel disease arthritis.
23. Infliximab Maintenance Therapy for Fistulizing Crohn`s Disease Background:
Infliximab , is effective in maintenance therapy for CD with no fistulae It is not known whether it is effective as maintenance therapy for patients with fistulae.
Methods:
Multicenter , double blind , randomized , placebo-controlled trial to evaluate the efficacy of infliximab maintenance therapy in 306 adult patients with CD & 1 or > draining abdominal or perianal fistulas of at least 3 months duration.
24. Cont� Patients received 5mg/kg, IV on weeks: 0 ,2 & 6.
A total of 195 patients who had a response at weeks 10 & 14 , and 87 patients who had no response were then randomly assigned to receive placebo or infliximab 5mg/kg every 8 weeks & to be followed to week 54.
The primary analysis was the time to loss of response among patients who had a response at week 14 and underwent randomization.
25. Results The time to loss of response was significantly longer for patients who received infliximab maintenance therapy than for those who received placebo ( more than 0 wks vs. 14 wks ) P= 0.001
At week 54 , 19% of patients in the placebo group had a complete absence of draining fistulas , as compared with with 36% of patients in the infliximab maintenance group. P = 0.009
26. Conclusion Patients with fistulizing CD who have a response at induction therapy with infliximab have an increased likelihood of a sustained response over 54-week period if infliximab treatment is continued every 8 weeks.
27. Methods Patients :
Men & women >18 yrs , with CD,1 or > fistula.
Concurrent therapies for CD were permitted .
Excluded :
abscess or stricture requiring surgery
Previously received infliximab
28. Methods Study design:
Patients were screened for eligibility 2 weeks before enrollment.
All eligible patients received Iv infusions 0,2 & 6 weeks
Response : reduction of at least 50% from baseline number of draining fistulas at consecutive visits 4 or > Wks apart.
Patient had a response if it was observed at both 10 & 14 wks.
29. Cont� Loss of response :
Recrudescence of draining fistulas.
Need to change medications for CD
Need for additional therapy for persistent or worsening luminal disease activity.
Discontinuation of study medication due to lack of efficacy .
Complete response : absence of fistulas