Download
1 / 1
10 likes | 92 Views
The short-term, between-session reproducibility of Sniff nasal pressure (SnPnas) in COPD patients; Implications for baseline measurements prior to rehabilitation programmes. Dimitra Nikoletou 1 , Gerard Rafferty 2 , Robert Grant 1 and John Moxham 2

E N D
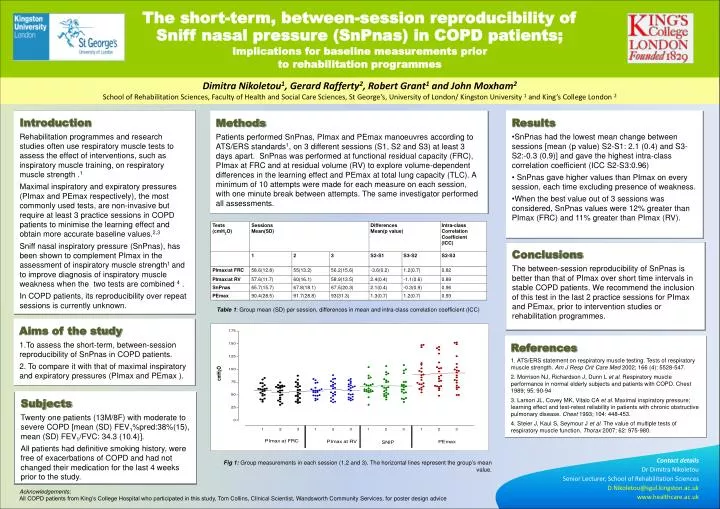
The short-term, between-session reproducibility of Sniff nasal pressure (SnPnas) in COPD patients; Implications for baseline measurements prior to rehabilitation programmes Dimitra Nikoletou1, Gerard Rafferty2, Robert Grant1 and John Moxham2 School of Rehabilitation Sciences, Faculty of Health and Social Care Sciences, St George's, University of London/ Kingston University1 and King’s College London 2 Introduction Rehabilitation programmes and research studies often use respiratory muscle tests to assess the effect of interventions, such as inspiratory muscle training, on respiratory muscle strength .1 Maximal inspiratory and expiratory pressures (PImax and PEmax respectively), the most commonly used tests, are non-invasive but require at least 3 practice sessions in COPD patients to minimise the learning effect and obtain more accurate baseline values.2,3 Sniff nasal inspiratory pressure (SnPnas), has been shown to complement PImax in the assessment of inspiratory muscle strength1 and to improve diagnosis of inspiratory muscle weakness when the two tests are combined 4. In COPD patients, its reproducibility over repeat sessions is currently unknown. • Results • SnPnas had the lowest mean change between sessions [mean (p value) S2-S1: 2.1 (0.4) and S3-S2:-0.3 (0.9)] and gave the highest intra-class correlation coefficient (ICC S2-S3:0.96) • SnPnas gave higher values than PImax on every session, each time excluding presence of weakness. • When the best value out of 3 sessions was considered, SnPnas values were 12% greater than PImax (FRC) and 11% greater than PImax (RV). Methods Patients performed SnPnas, PImax and PEmax manoeuvres according to ATS/ERS standards1, on 3 different sessions (S1, S2 and S3) at least 3 days apart. SnPnas was performed at functional residual capacity (FRC), PImax at FRC and at residual volume (RV) to explore volume-dependent differences in the learning effect and PEmax at total lung capacity (TLC). A minimum of 10 attempts were made for each measure on each session, with one minute break between attempts. The same investigator performed all assessments. Conclusions The between-session reproducibility of SnPnas is better than that of PImax over short time intervals in stable COPD patients. We recommend the inclusion of this test in the last 2 practice sessions for PImax and PEmax, prior to intervention studies or rehabilitation programmes. Table 1: Group mean (SD) per session, differences in mean and intra-class correlation coefficient (ICC) • Aims of the study • To assess the short-term, between-session reproducibility of SnPnas in COPD patients. • To compare it with that of maximal inspiratory and expiratory pressures (PImax and PEmax ). References 1. ATS/ERS statement on respiratory muscle testing. Tests of respiratory muscle strength. Am J RespCrit Care Med 2002; 166 (4): 5528-547. 2. Morrison NJ, Richardson J, Dunn L et al. Respiratory muscle performance in normal elderly subjects and patients with COPD. Chest 1989; 95: 90-94 3. Larson JL, Covey MK, Vitalo CA et al. Maximal inspiratory pressure; learning effect and test-retest reliability in patients with chronic obstructive pulmonary disease. Chest 1993; 104: 448-453. 4. Steier J, Kaul S, Seymour J et al. The value of multiple tests of respiratory muscle function. Thorax 2007; 62: 975-980. Subjects Twenty one patients (13M/8F) with moderate to severe COPD [mean (SD) FEV1%pred:38%(15), mean (SD) FEV1/FVC: 34.3 (10.4)]. All patients had definitive smoking history, were free of exacerbations of COPD and had not changed their medication for the last 4 weeks prior to the study. Contact details Dr Dimitra Nikoletou Senior Lecturer, School of Rehabilitation Sciences D.Nikoletou@sgul.kingston.ac.uk www.healthcare.ac.uk Fig 1: Group measurements in each session (1,2 and 3). The horizontal lines represent the group’s mean value. Acknowledgements: All COPD patients from King’s College Hospital who participated in this study, Tom Collins, Clinical Scientist, Wandsworth Community Services, for poster design advice