Download
1 / 19
190 likes | 379 Views
Cortex. Medulla. 90%. Pregn. Kynsterar. 10%. Sykursterar. Saltsterar. Barksterar. Adrenaline (85%) Noradrenaline. Tvö aðskilin stjórnkerfi. SYKUR. SALT. +. BST. Hippocampus. -. -. CRF AVP. AVP. AVP. +. CRF. Amygdala. PVN. SON. CBG. ?. +. -. -. AVP. ACTH. +.

E N D
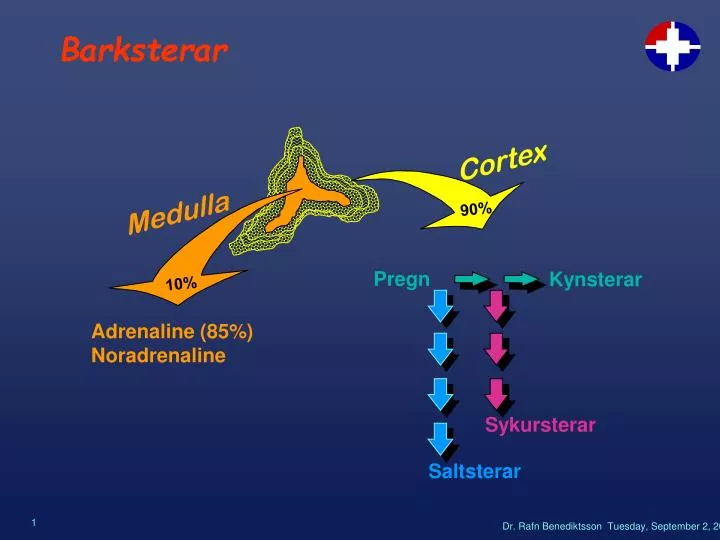
Cortex Medulla 90% Pregn Kynsterar 10% Sykursterar Saltsterar Barksterar Adrenaline (85%) Noradrenaline
Tvö aðskilin stjórnkerfi SYKUR SALT
+ BST Hippocampus - - CRF AVP AVP AVP + CRF Amygdala PVN SON CBG ? + - - AVP ACTH + 11b-HSD +? Heiladinguls-nýrnahettuöxullinn Type 1 Type 2
ACE A-I Angíótensínógen + A-II + + Renín ò s-K+ Aldósterón + SV - + ò þvag-Na+ñ þvag-K+ñ þvag-H+ òBÞ + (ACTH) Renín - Aldó - SV öxull
Orsakir nýrnahettubilunar • Prímer (Addison´s Disease) • Autoimmune • Uniglandular • Polyglandular • Sýkingar / sepsis • Meinvörp • Adrenomyeloneuropathy • Sekúnder • Sterameðferð • Æxli í heiladingli eða hypothalamus • Sheehan syndrome • Granuloma / hypophysitis • Skurðaðgerð / geislun
Addison Þreyta, slen og slappleiki Þyngdartap Réttstöðusvimi Lystarleysi - ógleði Kviðverkir - uppköst Saltfíkn Niðurgangur Heiladingulsæxli Staðbundin bitemporal hemianopia höfuðverkur brottfallseinkenni Almenn Ofgnótt hormóns Vöntun hormóns Einkenni við nýrnahettubilun
Skoðun Teikn prímer sjúkdóms Horaður og slappur einstaklingur Hyperpigmentation Axilla og pubis hártap Orthostatismi hypotensio CV-collapse Rannsóknir Hyponatraemia Hyperkalaemia Acidosis Hypoglycaemia Hypercalcaemia Hækkað urea Normochrome/cytic anaemia, lymphocytosis, eosinophilia Adrenal mótefni jákvæð Teikn sjúkdóms Addisons
A 55y old housewife is treated for hypothyroidismwith thyroxine 150mg/d but remains fatigued 3/12 later • Hb 112 g/l • MCV 103 fl • FT4 18 pmol/l • TSH 2.2 mU/l • Na+ 121 mmol/l • K+ 4.5 mmol/l • Cl- 97 mmol/l • U 8.9 mmol/l • BG 3.1 mmol/l • HCO3- 19 mmol/l • Why is she fatigued ? • What diagnostic test should be performed ? • Give two likely causes of the raised MCV
Greining • Grundvallarreglur efnaskiptalækninga • Grunur um skort è örvunarpróf • Grunur um ofgnótt è bælipróf • Synacthen próf • Samtengt ACTH (Tetracosactrin b1-24) • 250mg iv/im è s-kortisol @ 30 mín (ok > 550nM) • s-ACTH • Aldosterone og renín
Bráðameðferð • Meta vökvaástand. • Inf NaCl 0.9% hratt ± iv glúkósa 5-10%. • Inj. Hydrocortisone (kortisól) • 100mg iv stat svo 100mg x 3 iv (im). (Dexamethasone 4mg iv ef gert Synacthen próf) • Dagur 2 • Inj. Hydrocortisone 50mg x 3 iv (im). • Þegar borðar • Tabl. Hydrocortisone 20mg kl. 08 og 10mg kl.17. • Meta þörf á fludrocortisone. • Meðhöndla meðvirkandi/framkallandi sjúkdómsástand • Ath að gefa kortisól á undan T4 ef einnig hypothyroidism
Viðhaldsmeðferð • Langtíma uppbót per os • Hydrocortisone 10 - 20 mg mane og 5 - 10 mg kl 17. • Fludrocortisone 0,25 - 0,1 mg / d (einungis í 1°) • Uppbót við álag • Lítið è engin breyting • Meðal è tvöfaldur po skammtur þar til betri • Svæsið è iv eins og bráðameðferð • Periop kir minor è HCS 100 mg x 1 iv með pre-med kir major è HCS 100 mg x 3 iv aðgerðardag svo 50 mg x 3 næsta dag, síðan viðhald
Vandamál við uppbót kortisóls • Erfitt að bæla ACTH • Erfitt að líkja eftir eðlilegri kortisól dægursveiflu • Hefðbundnir HCS skammtar (30 mg / d) bæla osteocalcin
Er þörf á androgen uppbót ? • Dehydroepiandrosterone Replacement in Women with Adrenal Insufficiency. Arlt W et al. N Engl J Med 1999;341:1013-20 • Dehydroepiandrosterone (D) significantly improved overall well-being as well as scores for depression and anxiety. • For the global severity index, the mean (± sSD) change from base line was - 0.18 ± 0.29 after four months of D therapy, as compared with 0.03 ± 0.29 after four months of placebo (P = 0.02). • D increased the frequency of sexual thoughts (P = 0.006),sexual interest (P = 0.002), and satisfaction with both mental and physical aspects of sexuality (P = 0.009 and P = 0.02).
Ofgnótt Kortisóls • Cushing´s Syndrome • Ofgnótt kortisóls án tillits til orsakar - oftast afleiðing lyfjameðferðar • Cushing´s Disease • Ofgnótt kortisóls vegna ACTH framleiðandi æxlis í heiladingli
Hvaða teikn skipta máli • Discriminant Index • Bruising 10,5 • Myopathy 7,1 • Hypertension 5,1 • Plethora 3,6 • Oedema 3,3 • Red Striae 3,1Lancet 1982;2:646-649
Suspected Cushing’s Syndrome 1mg overnight dexamethasone testor 24h U free cortisol+ 48h low dose dexamethasone suppression +circadian plasma cortisol abstinence ? depression ? alcohol Confirmed Cushing’s Syndrome ITT Cushing’s syndrome: Establish the diagnosis
Cushing’s syndrome: Differential diagnosis Confirmed Cushing’s Syndrome ACTH DHEAS DA4 U/E’s BG Adrenal cause ACTH dependent CT adrenal +adrenal vein samplingradio-cholesterol scanningangiography CRH test & 48hhigh dose dexamethasonesuppression + inferiorpetrosal sinus sampling Ectopic source Pituitary source CXR, CT chest & abdomentumour markers + multiplevenous sampling for ACTH MRI Pituitary
Transsphenoidal skurðaðgerð Erfið tæknilega Geislameðferð 1/5 læknast á 1 - 14 árum 2/5 þurfa adrenalectomy Adrenalectomy 25% Nelson´s Syndrome Lyfjameðferð Metyrapone Ketoconazole Aminoglutethimide op-DDD Meðferð við Cushing´s Disease
