Download
1 / 37
370 likes | 539 Views
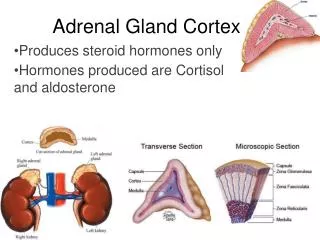
HORMONES OF THE ADRENAL CORTEX. Prof.Dr .Arzu Seven. HORMONES OF THE ADRENAL KORTEX. The adrenal c ortex makes 3 kinds of hormones : Mineralocorticoids Glucocorticoids Androgens.

E N D
HORMONES OF THE ADRENAL CORTEX Prof.Dr.Arzu Seven
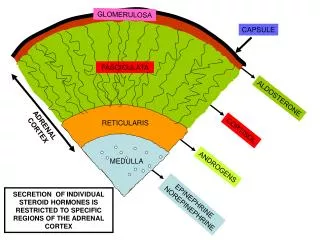
The adrenal cortexmakes 3 kinds of hormones: • Mineralocorticoids • Glucocorticoids • Androgens
There is an overlap of biologicalactivity, allnaturalglucocorticoidshavemineralocoticoidactivityandvice varsa • H + R (intracellular)gene expression
Chemicalstructure of steroidhormones: • 17-C cyclopentanoperhydrophenanthrenestructurewithfourringslabeled A_D • Additionalcarbons can be added at positions 10 or 13 or a sidechainattachedto C17 • Asymetriccarbonatomsallowforstereoisomerism
Glucocorticoids21C • Mineralocorticoids21C • Androgens19C • Estrogens18C
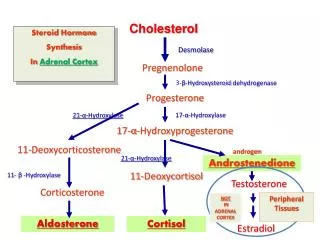
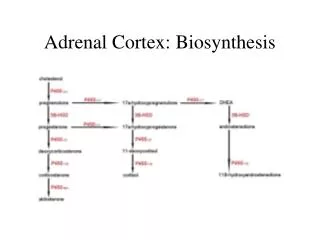
Synthesis of glucocorticoids • C17 • C21 • C11 • 17 • 21 • 11 hydroxylations Endoplasmicreticulum mitochondria
Cortisolis themajorglucocorticoid , synhesized in the adrenal cortex • It is underthedirectcontrol of pituitary ACTH • Cholestrol is theprecursorforallseroidhormones • Theconversion of cholestroltopregnenolone is the rate limiting step
Cleavage of thecholestrolsidechainliberatesC-21 corticosteroids, furthersidechaincleavageyields C-19 androgens, aromatization of ring A results in C-18 estrogens
Plazma concentrationshows a pronounceddiurnalrhythm, being 10 timeshigher at 08.00 hrthan at 24.00 hr • Thisparallelsthemarkeddiurnalrhythm of ACTH secretion • 95% of cortisol in plasma is boundtoproteins, mainlycorticosteridbindingglobulin(CBG) ortranscortin
CBG is produced in liver • Itssynthesis , like TBG, is increasedbyestrogens • Freefractionrepresentsthebiologicallyactivecortisol • Half life ~ 100 minutes
Inplasma :80% 17-OH corticoids, 20% cortisoneand 11-deoxycortisol metabolized in theliverbyreduction, sidechaincleavageandconjugationreactionslipophilicsteroidmoleculebecomeswatersolubleandexcretable
Inhumansmost of theconjugatedsteroids,thatentertheintestinebybiliaryexcretion,arereabsorbedbytheenterohepaticcirculation • Conjugatedsteroidsareexcreted : • 70% in theurine • 20%in thefeces • skin
Glucocorticoidhormonesaffectbasalmetabolism, hostdefencemechanism, bloodpressureandresponsetostress
Cortisolworks in tandem withinsulinand GH in regulatingintermediarymetabolism
Clinicaldisorders of cortisolsecretionhypofunction: • Hyposecretion of cortisolmayoccur as a result of hypothalamic,pituitaryor adrenal failure • Diagnosis: • Clinicalpresentation • Timedmeasurement of cortisoland ACTH • Extent of cortisolresponsetosynthetic ACTH (synacthen)
Addisondisease(adrenal insufficiency) • Primary adrenal failure autoimmune/infection(tbcorcytomegalivırus) • Secretion of all adrenal hormones
Biochemicalfeatures • Hyponatremia • Hyperkalemia • Acidosis • Urea • İmpairedcortisolresponsetosynacthen, togetherwith ACTH • Darkeningof skin andmucousmembranes • Hypovolemiaandhypotensionstimulate AVP secretionwaterretention
Synacthentests(shortorlong) • Synacthen is a synthetic,1-24 analogue of ACTH, adminsteredIV at a dose of 250µg • Cortisol is measured at 0,30,60 min • EquivocalorinadequateresponsestoSST (shortsynacthen test) mayrequire LST to be performed in ordertoestablishwhether adrenal insufficiency is primaryorsecondarytopituitaryorhypothalamicdisease.DepotSynacthen (1mg) is given IM for 3 days SST repeatedon the 4th day
A normal responsemakesprimary adrenal insufficiencyunlikely • LST may not be neededwhen ACTH is measured
Therapy:cortisolreplacament , usuallytogetherwith a mineralocorticoid • Addison’sdisease can be associatedwithelevated TSH whichrevolveswithglucocorticoidtherapy
hyperfunction • Hypersecretion of cortisolresults in Cushing’ssyndrome • Prolongeduse of exogenousglucocorticoids (iatrogenic) • Disordersthehypothalamus, pituitary (80%) or adrenal gland(15%) • Ectopic ACTH syndrome
Cortisolexcessproduces DM andhypertension, andusuallysuppressesthehypothalamicgonadalaxis (amenorrhea)
diagnosis • Randommeasurement of cortisol is of littleusebecause of thepronouncedcircadianvariation • 24 hoururinaryfreecortisolorcortisol/creatinineratio in an earlysample is a commonscreening test • Repeatedlyhighearlymorningurinecortisol /creatinineratiosindicatefurtherinvestigations • Ifthe test is negative on 3 occasionsexcludeCushing’ssyndromefromdifferentialdiagnosis
Cortisolconcentrations at 08.00 and 22.00 normallyshows a circadianrhythmwitheveningsamplehaving a lowervaluethan in themorning • Loss of thisrhythmindicatesCushing’ssyndrome • Failure of 1 mg dexamethasonetaken at 23.00 tosupress serum cortisollevel at 08.00 thefollowingmorning, orfailuretosupressurinarycortisolsecretionovernight (cortisol/creatinine) is anotherindicator of Cushing’ssyndrome
Failure of serum cortisoltoriseafterinsulin_inducedhypoglycaemia(0.15 unitsinsulin /kg) is a characteristicfeature of Cushing’ssyndrome • InpatientswithpitiutarydependentCushing’sdisease , serum urinarycortisolwill be partiallysupressedafter 2 days of dexamethasone, 2.0 mg q.i.d. (syntheticglucocorticoid) • Failuretosupresssuggestseitherectopic ACTH productionorautonomoussecretion of cortisolby an adrenal tm