Download
1 / 28
280 likes | 384 Views
DEPRESSION IN MEDICAL SETTINGS: STRATEGIES FOR INTEGRATION. Steven Cole, MD Professor of Clinical Psychiatry S.U.N.Y. Stony Brook Health Sciences Center Rural Quality Program Conference, Office of Rural Health Policy Health Resources Services Administration September 1, 2009.

E N D
DEPRESSION IN MEDICAL SETTINGS: STRATEGIES FOR INTEGRATION Steven Cole, MD Professor of Clinical Psychiatry S.U.N.Y. Stony Brook Health Sciences Center Rural Quality Program Conference, Office of Rural Health Policy Health Resources Services Administration September 1, 2009
DEPRESSION IN MEDICAL PATIENTS IS COMMON • 20-50% of patients w/diabetes, CAD, PD, MS, CVA, asthma, cancer... (etc) have MD • Prevalence varies by illness, pathophysiology, severity, and research methodology • Depressed patients visit PCPs 3x more often than patients not depressed
DEPRESSION IS SIGNIFICANT • Increased morbidity and mortality in medical conditions • Increased utilization • Increased costs • 4th leading cause of disability worldwide (2nd in 2020)
GLOBAL BURDEN OF DISEASE: WORLD HEALTH ORGANIZATION • 1990 • Lower respiratory infection • 2 Conditions arising during the perinatal period • 3 Diarrheal diseases • 4 Unipolar major depression • 5 Ischemic heart disease • 6 Vaccine-preventable disease • 2020 • Ischemic heart disease • Unipolar major depression • Road traffic accidents • Cerebro-vascular disease • Chronic obstructive pulmonary disease • Lower respiratory infections Murray & Lopez, WHO: Global Burden of Disease, 1996; Michaud, JAMA, 2001
Depressed (n=35) Nondepressed (n=187) Cox Hazard Ratio = 5.74 p=0.0006 Frazure-Smith, JAMA 1993;270:1819-1825 Circulation 1995;91:999-1005
DEPRESSION IN CARDIAC DISEASE • risk of hypertension; CVA; CAD • death risk after MI (controlling for other risks) • HPA activation • sympatho-medullary activity • platelet aggregation; HR variability • Musselman et al Archives Gen Psych 1998 • van Kanel et al Psychosom Med 2001
DEPRESSION IN DIABETES • non-adherence • GHb • retinopathy; neuropathy; nephropathy • macrovascular complications (CAD, etc) • Groot et al Psychosom Med 2001 • Van Tilburg et al Psychosom Med 2001
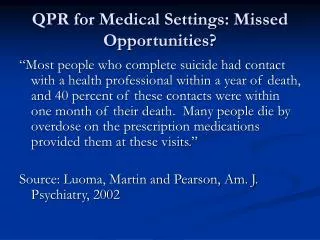
UNDER-RECOGNITION/UNDERTREATMENT • 30%-70% of depression missed • 50% stop medication in 3 months • 50% of treatedpatients in primary care remain depressed after 1 year
PATIENT HEALTHQUESTIONNAIRE: (PHQ) • 9-item, self-administered questionnaire • Validated for diagnostic assessment • Validated for follow-up of outcomes • Clinically significant depression (“CSD”): PHQ = 10 or greater
SCORING THE PHQ: DIAGNOSTIC ASSESSMENT Count numerical values of symptoms • 0-4 not clinically depressed • 5-9 mild depressive symptoms or... • adjustment disorder • dysthymic disorder • 10-14 mild/moderate depression • CSD (88% sens/spec for major depression) • >14 mod/severe depression
USE OF THE PHQ • Assess high-risk, ‘red flag’ patients • Chronic illness • Unexplained physical complaints • Patients who appear sad/ stressed • Patients who have lost interest or pleasure in their lives
MANAGEMENT GUIDELINES I: Acute Phase • Start with medication or psychotherapy • Elicit commitment to take medication or attend therapy regularly (action plan) • Arrange early (1-3 week) follow-up • Repeat PHQ every 1-2 months • Re-evaluate treatment every month depending on PHQ score (adjust meds; adjust therapy)
OUTCOME TARGETS: DEFINITIONS • “Clinically significant improvement (CSI)” • 5 point decrease in PHQ score • “Response” • 50% decrease in PHQ score • “Remission” • PHQ score <5 for three months
SELF-MANAGEMENT SUPPORT • Integrate SMS into routine care in all visits • Three minute goal-setting (SMS) • Goal 1: “Are you willing to take this every day?” • “What is your confidence on a 1 to 10 scale that you will actually take the medicine every day?” • Goal 2: “To make sure the medicine is working, we need to see you again (or talk by phone) in a week or so.” • “What is your confidence that you will make it for this visit (or phone call) that we agreed to?” • Chart Note • “PAP: agrees to take meds regularly (cl = 8)” • “PAP: agrees to return for visit in 2 weeks (cl=7)”
Early Steps in Depression Care Activities in the Six Components of the Care Model Dan Ford, MD
Unique Aspects of Depression • Depression is a chronic relapsing condition (like asthma) • Depressive symptoms closely linked with function in time • Diagnosis and monitoring based on self-report, not labs or exam (telephone is ideal)
Unique Aspects of Depression • Depression itself may interfere with patient’s self-care planning • Overly pessimistic about effectiveness of treatment • Difficulty monitoring oneself and making decisions
Unique Aspects of Depression • Social stigma • Health personnel have varying degree of comfort with depression • Largest gulf between primary care providers and specialists in depression • Depression care may be reimbursed/funded at lower level than other chronic conditions
First Steps: Depression Self Management • Examine the patient handouts provided (e.g. Depression Self-Action Plan) • Try these materials out with a sample of patients and determine how they might have to be adapted for patients with chronic medical conditions
First Steps: Decision Support • Identify one or two local mental health specialists to help support your depression treatment program (medications and psychotherapy) • Let cluster directors know if not successful • Develop a suicide protocol • Train staff in suicide assessment • Establish referral protocols
First Steps: Clinical Information Systems • Learn how to enter PHQ scores in registry • Learn how to interpret longitudinal PHQ scores for patients • Maximize efficiency in data entry
First Steps: Delivery System Design • Identify one person on team to be the champion for depression care • Integrate depression education into other programs
First Steps: Organization of Health Care • Identify what resources will be needed for the depression care program • Identify and address any objections from senior leaders and staff members to expanding care to depression • Common barriers include: 1) our patients do not want to address depression; 2) somatic care is more important; 3) we do not have the right staff; 4) our patients need help with social and economic issues, not depression
First Steps: Community • Begin to identify community resources for patients with depression • Local • National • National Depressive and Manic-Depressive Association www.ndmda.org • National Mental Health Association www.nmha.org
8 Early Steps 1. Identify a mental health specialist 2. Develop a suicide protocol 3. Develop initial antidepressant guidelines 4. Integrate SMS (‘ultra-brief personal action plan’) into clinical practice/select a SMS tool
Eight early steps 5. Administer the PHQ to two patients suspected to have depression 6. Initiate antidepressant protocol and ultra-brief PAP/SMS tool 7. Repeat PHQ at one month and two months 8. Review results with team - PDSA