Download

1 / 53
540 likes | 600 Views
DIPHTHERIA. Dr. PRACHETH R. Outline. Introduction Magnitude Epidemiology Clinical features Treatment Prevention and Control. Introduction. Greek language : leather Under five Corynebacterium diphtheriae Gradual rise of temperature Greyish-yellow membrane: throat, tonsils.

E N D
DIPHTHERIA Dr. PRACHETH R.
Outline • Introduction • Magnitude • Epidemiology • Clinical features • Treatment • Prevention and Control
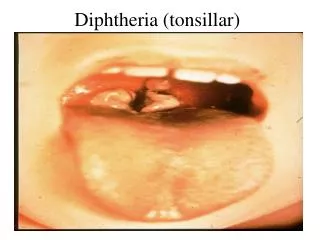
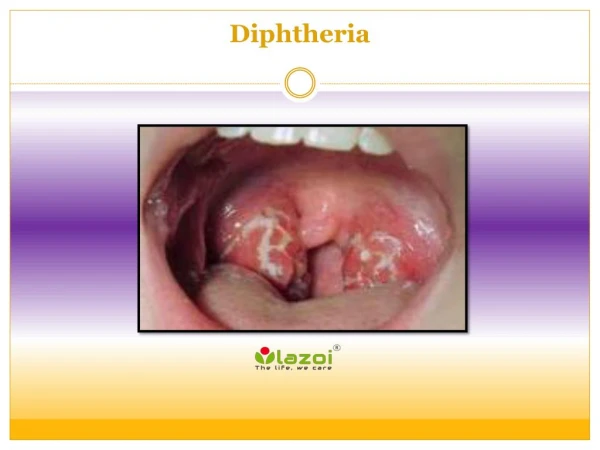
Introduction • Greek language : leather • Under five • Corynebacteriumdiphtheriae • Gradual rise of temperature • Greyish-yellow membrane: throat, tonsils
Magnitude of the problem • Almost eliminated: developed countries-mass immunization • India: lack –adequate immunization • Around: 4,286 cases and 112 deaths
Agent factors Agent: Corynebacterium diphtheria • Gram-positive , non-capsulated, non-spore forming bacillus. • Appear in pairs, lying: angles- Chinese letter • No invasive power, powerful toxin
Agent factors Reservoir of infection: man • Human: case/ carrier • Every clinical case: 10 carriers • Temporary or chronic carrier • Nose, throat • Cutaneous >respiratory
Agent factors • Infective materials: nasopharyngeal secretions, discharges: cutaneous lesions, fomites, dust • Period of infectivity: From 2-4 weeks Chronic carriers: one year
Host factors Age incidence: High between 1-5 years • Less in< 6 months • Shift: preschool to school age Gender: equal Immunity: Almost 70 percent: subclinical infection. • More than 85% coverage: herd immunity
Environmental factors • Highest in winter season: indoor life, overcrowding
Modes of transmission • Droplet mode: commonest • Direct contact: cutaneous diphtheria • Indirect: fomites- handkerchiefs, pens, plates, cups
Portal of entry • Commonest: respiratory tract • Occasionally: abraded skin, mucous membrane
Pathology and pathogenesis • Respiratory tract: inhalation • Implant: upper respiratory passage- tonsils, nasopharynx or larynx, multiply-inflammatory reaction • No circulation: no invasive power • Exotoxin: circulation- toxaemia: necrosis • Fibrin clots, necrosed cells (dead/living bacilli, leucocytes): pseudo-membrane (greyish yellow)
Pathology and pathogenesis • They reach lymph nodes: enlarged, tender • Exotoxin: fixed- heart , cranial nerves (glossopharyngeal) • Myocarditis, heart failure • Palatal paralysis, nasal regurgitation • Toxin: lose toxicity-few months
Clinical features • Incubation period: 2-6 days • Disease begins quietly • Gradual rise of temperature, headache, body ache, malaise • Specific features: type
Clinical features Pharyngotonsillar: sore throat, low grade fever, difficult swallowing • Pseuodmembrane • Severe: oedema –submandibular, lymphadenopathy: bull neck Laryngotracheal: hoarseness, fever, cough, dyspnoea
Clinical features • Nasal: mildest form • Cutaneous: secondary infection: abrasion • Patients: seek treatment-lesion
Control of diphtheria Cases and carriers: • Early detection: • Active search: family, school contacts • Swabs: nose, throat • Carriers: culture • Isolation: • At least 14 days • Two consecutive swabs, 24 hours apart
Control of diphtheria • Treatment: • Cases: • Diphtheria Antitoxin : IM/IV -20,000 to 100,000 units • Preliminary test dose: 0.2 ml SC • Mild , early pharyngeal: 20,000-40,000 • Moderate nasopharyngeal: 40,000-60,000 • Severe: 80,000-100,000. • Penicillin/erythromycin: 5-6 days
Control of diphtheria • Carriers: • Ten day : oral erythromycin Contacts • Within 2 years : no action • More than 2 years: booster dose • Non-immunized: prophylactic penicillin/erythromycin, 1000-2000 units • Medical surveillance: one week, bacteriological: several weeks
Control of diphtheria Community: • Active immunization as per National Immunization Schedule • Immunize: maternal immunity lost • Does not prevent carrier state
Vaccination • Combined vaccines • Single vaccines • Antisera: Diphtheria Antitoxin
DPT vaccine (Triple Antigen) • Killed , bacterial , liquid vaccine • Dose: 0.5 ml • Antero-lateral aspect of thigh • Reactions: pain, fever: next day. Rarely: anaphylactic shock, convulsions • Contraindications: convulsions, reaction to previous dose • Storage: 2-8 degree C
DPT vaccine • Instructions: • Report if child develops reactions • Report for next dose • Complete schedule positively
Pentavalent vaccine • Five individual vaccines conjugated in one
Whooping cough Dr. Pracheth R
Objectives • Explain epidemiology • Enumerate control measures
Outline • Introduction • Problem statement • Epidemiology • Clinical features • Control
Introduction • Acute infectious, young children • B. pertussis • Insidious onset, mild fever, irritating cough • Gradually: paroxysmal- whoop (loud crowing inspiration) • Severe-atypical without whoop • Hundred Day Cough
Problem Statement • 1.29 Lakh cases globally • Most lethal: those not immunized • Underlying malnutrition, respiratory infections • India: decline • Cases: 39,091.
Epidemiology-Agent factors • Agent: • Most: B.pertussis • Small (5%): B.parapertussis • Certain viruses (Adenovirus, Parainfluenza viruses)
Agent factors • Source of infection: • Infects only man • Source: case • No evidence: subclinical, chronic carrier state • Infective material: • Bacilli: abundant- nasopharyngeal, bronchial secretions • Contaminated objects.
Agent factors • Infective period: • Most infective: catarrhal stage • Week after exposure-3 weeks after onset-paroxysmal stage-diminish after catarrhal • Secondary Attack Rate: 90%- unimmunized contacts
Host factors • Age: • Disease: infants, children • Below 6 months: highest deaths • Older children: atypical course • Sex: • Incidence, fatality: female>males.
Host factors • Immunity: • Recovery/ adequate immunization: followed by immunity • Second attacks usually mild • Infants susceptible from birth • No cross immunity.
Environmental factors • Throughout the year • Seasonal trend: more cases-winter • Overcrowding • Socio-economic status.
Mode of transmission • Spreads: droplet infection, direct contact • Fomites: very small. Incubation period: • 7-14 days
Clinical features • Local infection; organism: not invasive • Multiplies: surface epithelium-respiratory tract • Inflammation, necrosis of mucosa • Secondary bacterial invasion
Clinical features Catarrhal stage: • Lasts: 10 days • Insidious onset, sneezing, lacrimation Paroxysmal stage: • Lasts 2-4 weeks • Rapid cough, deep high-pitched inspiration (whoop) Convalescent stage: 1-2 weeks
Control Cases: • Early diagnosis, treatment, isolation • Bacteriological examination: nose and throat secretions: nasopharyngeal swab • Fluorescent antibody technique • Patient isolated: non-infectious • Erythromycin: 30-40mg/kg, 4 divided doses-10 days
Control • Paroxysmal stage: antibiotics-no change clinical course • Eliminate bacteria –nasopharynx Contacts: • Young children: away • Erythromycin/ampicillin-10 days • Infant: DPT best protection
DPT vaccine (Triple Antigen) • Killed , bacterial , liquid vaccine • Dose: 0.5 ml • Antero-lateral aspect of thigh • Reactions: pain, fever: next day. Rarely: anaphylactic shock, convulsions • Contraindications: convulsions, reaction to previous dose • Storage: 2-8 degree C
Pentavalent vaccine • Five individual vaccines conjugated in one