Download
1 / 9
100 likes | 228 Views
The Referenced EEG. A patient’s pretreatment QEEG data is obtained and statistically compared with similar QEEG data from patients with known medication responsivity. The result is a prediction of the patient’s likely responsivity to particular medications.

E N D
The Referenced EEG • A patient’s pretreatment QEEG data is obtained and statistically compared with similar QEEG data from patients with known medication responsivity. • The result is a prediction of the patient’s likely responsivity to particular medications. • This, in turn, informs the treatment strategy for the patient.
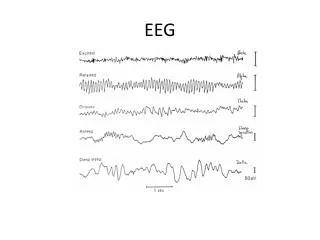
The rEEG Conjecture • Resting EEG is stable • Resting EEG Changes with Medications • Use Medications to normalize the EEG • Normalized EEG leads to normalized behavior
Database Comparison • Normal Subject Database: • 2082 QEEG’s, Subjects 6-90 • Original Pharmacotherapy Outcome Database • 1600 patients followed for at least 26 wks • 84 medications tracked for effectiveness over more then 6000 treatment episodes • 8467 patient follow-up assessments • Outcome assessment using clinical Global Improvement scale (CGI)
When appropriately medicated, abnormal brain function can be improved or normalized Patient 1:Pre and Post Treatment Z score (degree of abnormality)
Using rEEG, medications are selected which affect neurophysiology in known ways Patient 2: Pre-treatment Z score (degree of abnormality)
Medications that are not compatible for a neurophysiology* can yield iatrogenic illness Patient 2: Pre and Post treatment Z score (degree of abnormality) * Frequently occurs with symptom/behavioral-based treatment selection
Monte Nido Treatment Center • 84 Eating Disorder Patients Treated by rEEG Protocols After 8 weeks • 80% (29/36) Anorexia Nervosa patients responded • 83% (30/36) Bulimia Nervosa patients • 89% (8/9) EDNOS
EEG Guidance of Psychopharmacologic Treatment: Multi-Site ExperienceMark J. Schiller, M.D., W. Hamlin Emory, M.D., Jay Shaffer, M.D., James T. Hamilton, M.D., Daniel A. Hoffman, M.D., Albert Davis, M.D., Stephen S. Suffin, M.D.APA May 2005 Scientific Poster - 500 patients
Who is not suitable? • Under 6 or over 90 years old • Intramuscular depo-neuroleptic therapy within the preceding twelve months • History of craniotomy (with or without metal prostheses) or cerebral vascular accident • Spikes on the conventional EEG • Current diagnosis of seizure disorder or dementia • Mental retardation • Current use of marijuana; cocaine, hallucinogens or other drugs of abuse or alcohol in the last three days • Significant abnormality of the CBC, chemistry or thyroid function tests including TSH until corrected