Download
1 / 1
20 likes | 196 Views
Simultaneous UPLC-TMS assay for the detection of Levetiracetam and Gabapentin in serum and plasma. K. Johnson-Davis 1,2 , J.M. Juenke 1 , P.I. Brown 1 , G.A. McMillin 1,2 1 ARUP Institute for Clinical and Experimental Pathology, Salt Lake City, UT, 2 Department of Pathology,

E N D
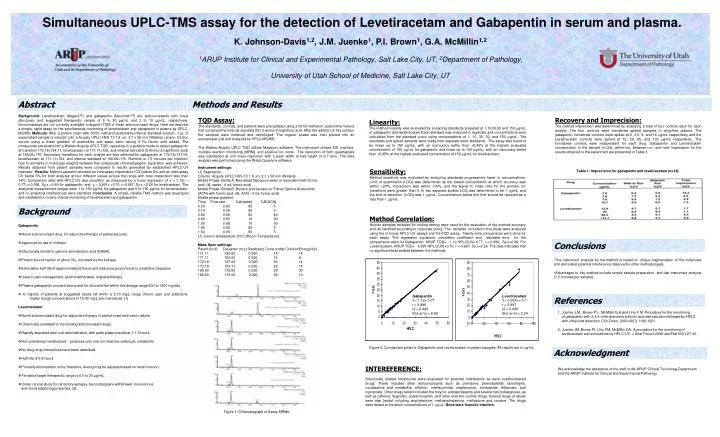
Simultaneous UPLC-TMS assay for the detection of Levetiracetam and Gabapentin in serum and plasma. K. Johnson-Davis1,2, J.M. Juenke1, P.I. Brown1, G.A. McMillin1,2 1ARUP Institute for Clinical and Experimental Pathology, Salt Lake City, UT, 2Department of Pathology, University of Utah School of Medicine, Salt Lake City, UT Abstract Methods and Results Background: Levetiracetam (KeppraTM) and gabapentin (NeurontinTM) are anticonvulsants with novel structures, and suggested therapeutic ranges of 5 to 30 µg/mL and 2 to 10 µg/mL, respectively. Immunoassays are not currently available to support TDM of these anticonvulsant drugs. Here we describe a simple, rapid assay for the simultaneous monitoring of levetiracetam and gabapentin in plasma by UPLC-MS/MS. Methods: After a protein crash with 50:50 methanol:acetonitrile internal standard solution, 1 µL of supernatant sample is injected onto a Acquity UPLC HSS T3 1.8 um, 2.1 x 50 mm (Waters) column. Elution occurs using a linear gradient of acetonitrile and water each having 0.1% formic acid added. The compounds are eluted into a Waters Acquity UPLC TQD, operating in a positive mode to detect gabapentin at transition 172.18>154.11, levetiracetam at 171.11>126, and internal standard (3-Amino-2-naphtholic acid) at 188.06>170. Secondary transitions for each analyte are also detected for gabapentin at 172.18>137.06, levetiracetam at 171.11>154, and internal standard at 188.06>115. Runtime is 1.5 minutes per injection. Due to similarity in molecular weights between the compounds chromatographic separation was achieved. Results obtained from patient samples were compared to results generated by established HPLC-UV methods. Results: Method validation showed an intra-assay imprecision (CV) below 8% and an inter-assay CV below 5% for both analytes at four different values across the range with total imprecision less than 14%. Comparison data with HPLC-UV was excellent, as measured by a linear regression of y = 1.12x – 0.77, r=0.996, Sy,x =0.89 for gabapentin, and y = 0.991x +0.70, r=0.997, Sy,x =2.24 for levetiracetam. The analytical measurement ranges were 1 to 150 µg/mL for gabapentin and 5 to 150 µg/mL for leviteracetam, and no analytical interferences were identified. Conclusion: A simple, reliable TMS method was developed and validated for routine clinical monitoring of levetiracetam and gabapentin. TQD Assay: The standards, controls, and patients were precipitated using a 50:50 methanol: acetonitrile mixture that contained the Internal standard (IS) 3-amino-2-naphthoic acid. After the addition of this solution the samples were vortexed and centrifuged. The organic phase was then poured into an autosampler vial and analyzed by HPLC-MS/MS. The Waters Acquity UPLC TQD ulilizes Masslynx software. The instrument utilizes ESI interface, multiple reaction monitoring (MRM), and positive ion mode. The resolution of both quadrapoles was maintained at unit mass resolution with a peak width at half height of 0.7 amu. The data analysis was performed using the Water Quanlynx software. Linearity: The method linearity was evaluated by analyzing standards prepared at 1,10,30,50 and 150 g/mL of gabapentin and levetiracetam Each standard was analyzed in duplicate and concentrations were calculated from the standard curve using concentrations of 1, 10, 30, 50, and 150 g/mL. The standards and spiked samples were made from separate stock standards. The assay was found to be linear up to 150 g/mL, with an inaccuracy better than 0.45% at the highest evaluated concentration of 150 g/mL for gabapentin and linear up to 150 g/mL, with an inaccuracy better than 0.25% at the highest evaluated concentration of 150 g/mL for levetiracetam. Recovery and Imprecision: The method imprecision was determined by analyzing a total of four controls each for each analyte. The four controls were homebrew spiked samples in drug-free plasma. The gabapentin homebrew controls were spiked at 2, 3.5, 8, and 16 g/mL respectively and the Levetiracetam controls were spiked at 12, 20, 65, and 100 g/mL respectively. The homebrew controls were independent for each drug. Gabapentin and Levetiracetam concentration in the sample (n=24), within-run, between-run, and total imprecision for the results obtained in the experiment are presented in Table 1. Instrument settings: LC Seperation: Column: Acquity UPLC HSS T3 1.8 um, 2.1 x 50 mm (Waters) Mobile Phase: Bottle A: Barnstead Nanopure water or equivalent with formic acid. (4L water : 4 mL formic acid) Mobile Phase: Bottle B: Burdick and Jackson or Fisher Optima Acetonitrile (ACN) with formic acid. (4L ACN : 4 mL formic acid) Mobile phase gradient: Time` Flow rate %A(water) %B(ACN) 0.00 0.65 95 5 0.10 0.65 95 5 0.80 0.65 60 40 0.85 0.65 10 90 1.00 0.65 10 90 1.05 0.65 95 5 1.50 0.65 95 5 LC column temperature: 24C (Room Temperature). Mass Spec settings: Parent (m/z) Daughter (m/z) Dwell(sec) Cone (volts) CollisionEnergy(eV) 171.11 126.00 0.020 14 14 171.11 154.00 0.020 14 8 172.18 137.06 0.020 26 14 172.18 154.11 0.020 26 14 188.00 115.00 0.020 23 30 188.00 170.00 0.020 23 10 Table 1: Imprecision for gabapentin and levetiracetam (n=24) Sensitivity: Method sensitivity was evaluated by analyzing standards progressively lower in concentrations. Limit of quantitation (LOQ) was determined as the lowest concentration at which accuracy was within 20%, imprecision was within 15%, and the signal to noise ratio for the primary ion transitions were greater than 5. In two separate studies LOQ was determined to be 1 g/mL and the limit of detection (LOD) was 1 g/mL. Concentrations below this limit should be reported as a less than 1 g/mL. Background Method Correlation: Human samples received for routine testing were used for the evaluation of the method accuracy and de-identified according to corporate policy. The samples included in this study were analyzed using the in house HPLC-UV assays and the TQD assay. Twenty-nine comparisons were done for each assay. The regression equations, correlation coefficient and standard error for the comparisons were for Gabapentin: ARUP TQD= 1.12 HPLC(UV)-0.77, r = 0.996, Sy,x=0.89. For Levetiracetam: ARUP TQD= 0.991 HPLC(UV)+0.70, r = 0.997, Sy,x=2.24. The data indicated that no significant bias existed between the methods. • Gabapentin: • Novel anticonvulsant drug for adjunctive therapy of partial seizures. • Approved for use in children. • Structurally similar to gamma-aminobutyric acid (GABA). • Protein bound fraction of about 3%, excreted via the kidneys • Elimination half-life of approximately 6 hours and clearance proportional to creatinine clearance • Used in pain management, alcohol withdrawal, migraine therapy • Plasma gabapentin concentrations and for clinical effect within the dosage range 600 to 1800 mg/day. • A majority of patients at suggested doses fall within a 2-10 mg/L range chronic pain and addictions higher trough concentrations of 15-30 mg/L are maintained. (1) • Levetiracetam: • Novel anticonvulsant drug for adjunctive therapy in partial-onset seizures in adults • Chemically unrelated to the existing anticonvulsant drugs. • Rapidly absorbed after oral administration, with peak plasma levels at 1-1.5 hours. • Not extensively metabolized - produces only one non-reactive carboxylic metabolite. • No drug-drug interactions have been described. • Half-life of 6-8 hours • Primarily eliminated in urine; therefore, dosing may be adjusted based on renal function. • Tentative target therapeutic range is 6.0 to 20 µg/mL. • Under clinical study for refractory epilepsy, benzodiazepine withdrawal, monoclonus, and mood stabilizing properties. (2) Conclusions • The instrument analysis by the method is based on unique fragmentation of the molecules and eliminates potential interference observed in other methodologies. • Advantages to this method include simple sample preparation, and fast instrument analysis (1.5 minutes per sample). Gabapentin Y= 1.12x-0.77 r = 0.996 r2 = 0.992 Std. error = 0.89 Levetiracetam Y= 0.991x+-0.7 r = 0.997 r2 = 0.996 Std. error = 2.24 References 1. Juenke J.M., Brown P.I., McMillin G.A.and Urry F.M. Procedure for the monitoring of gabapentin with 2,4,6-trinitrobenzene sulfonic acid derivatization followed by HPLC with ultraviolet detection. Clin Chem, 2003 49(7) 1198-1201. 2. Juenke JM, Brown PI, Urry FM, McMillin GA. A procedure for the monitoring of levetiracetam and zonisamide by HPLC-UV. J Anal Toxicol 2006 Jan/Feb 30(1):27-30. Figure 2: Comparison plots for Gabapentin and Levetiracetam in patient samples. All results are in g/mL. Acknowledgment INTEREFERENCE: Structurally related compounds were evaluated for potential interference as were coadministered drugs. These included other anticonvulsants such as primidone, phenobarbital, lamotrigine, oxcarbazine and metabolite, ethotoin, methsuximide, mephenytoin, zonisamide, felbamate, and topiramate. Other drugs tested included the tricyclic antidepressants and several benzodiazepines, as well as caffeine, ibuprofen, acetaminophen, and other over the counter drugs. Several drugs of abuse were also tested including amphetamine, methamphetamine, methadone and cocaine. The drugs were tested at the stock concentrations of 1 g/L. None were found to interfere. We acknowledge the assistance of the staff in the ARUP Clinical Toxicology Department and the ARUP Institute for Clinical and Experimental Pathology Figure 1: Chromatograph of Assay MRMs.