Download
1 / 12
120 likes | 275 Views
What form of anticoagulation is the “best ”. Or why is Citrate better then Heparin or Prostacyclin . Anticoagulation and clotting . Any blood surface interface Hemofilter Bubble trap Catheter Areas of turbulence resistance Luer lock connections / 3 way stopcocks.

E N D
What form of anticoagulation is the “best” Or why is Citrate better then Heparin or Prostacyclin
Anticoagulation and clotting • Any blood surface interface • Hemofilter • Bubble trap • Catheter • Areas of turbulence resistance • Luer lock connections / 3 way stopcocks
Sites of Action of Citrate Contact Phase (intrinsic) XII activation XI IX Ca++ Tissue Factor (extrinsic) TF:VIIa platelets / monocytes / macrophages Va VIIIa Ca++ platelets X Xa prothrombin Citrate CITRATE THROMBIN Ca++ fibrinogen CLOT
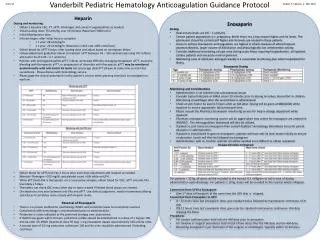
Solutions needed for Citrate Protocol(Pediatric Nephrology 2002 17:150-154 ) • ACD-A (Baxter, Deerfield, IL) • 1000 cc bag, industry standard • CaCl 8 gms/1 liter of NS • pharmacy made • Normocarb Dialysis/Replacement Soln (Dialysis Soln Inc) • Can be prepared at bedside or pharmacy • Normal Saline
(Ca = 0.4 x citrate rate 60 mls/hr) (Citrate = 1.5 x BFR 150 mls/hr) Pediatr Neph 2002, 17:150-154 (BFR = 100 mls/min) Normal Saline Replacement Fluid Calcium can be infused in 3rd lumen of triple lumen access if available. Normocarb Dialysate • ACD-A/Normocarb Wt range 2.8 kg – 115 kg • Average life of circuit on citrate 72 hrs (range 24-143 hrs)
Citrate: Technical Considerations • Measure patient and system iCa in 2 hours then at 6 hr increments • Standing protocol on nursing flow sheet adjusted by bedside ICU nurse • Pre-filter infusion of Citrate • Aim for system iCa of 0.25-0.4 mmol/l • Adjust for levels • Systemic calcium infusion • Aim for patient iCa of 1.1-1.3 mmol/l • Adjust for levels
Seven ppCRRT centers • 138 patients/442 circuits • 3 centers: hepACG only • 2 centers: citACG only • 2 centers: switched from hepACG to citACG • HepACG = 230 circuits • CitACG= 158 circuits • NoACG = 54 circuits • Circuit survival censored for • Scheduled change • Unrelated patient issue • Death/witdrawal of support • Regain renal function/switch to intermittent HD
ppCRRT ACG Side Effects • Heparin • 11 cases of systemic bleeding on heparin • 5 cases no ACG used secondary to bleeding • 1 case of HIT • Citrate • 19 cases of metabolic alkalosis • 1 change to heparin for hyperglycemia • 1 change to heparin for alkalosis • 3 cases of citrate lock
Complications of Citrate: • Citrate Lock • Seen with rising total Ca with dropping patient ionized Ca due to citrate delivery exceeds citrate clearance • Rx of “citrate lock” • Increase clearance and decrease citrate rate • Metabolic Alkalosis • Resolved with NaHCO3 bath of 25 meq/l
Incidence • In a recent survey of PICU and CRRT databases in NA 70% of all programs use citrate as a primary mode of anticoagulation to avoid bleeding risks