Download
1 / 1
10 likes | 160 Views
I. HPP. Thailand. National Health Accounts in Thailand 1994-2005. Kanjana Tisayatikom, Walaiporn Patcharanarumol, Artidtaya Tiampraiwan, Hathaichanok Sumalee, Phusit Prakongsai, Viroj Tangcharoensathien International Health Policy Program (IHPP) – Thailand. BACKGROUND :

E N D
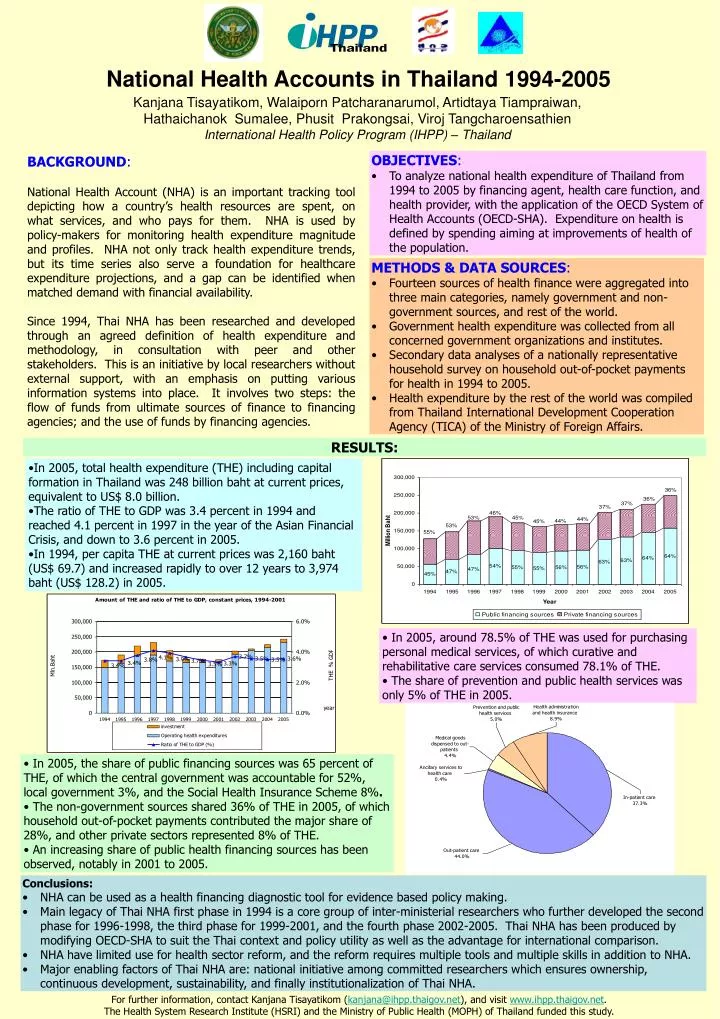
I HPP Thailand National Health Accounts in Thailand 1994-2005 Kanjana Tisayatikom, Walaiporn Patcharanarumol, Artidtaya Tiampraiwan, Hathaichanok Sumalee, Phusit Prakongsai, Viroj Tangcharoensathien International Health Policy Program (IHPP) – Thailand BACKGROUND: National Health Account (NHA) is an important tracking tool depicting how a country’s health resources are spent, on what services, and who pays for them. NHA is used by policy-makers for monitoring health expenditure magnitude and profiles. NHA not only track health expenditure trends, but its time series also serve a foundation for healthcare expenditure projections, and a gap can be identified when matched demand with financial availability. Since 1994, Thai NHA has been researched and developed through an agreed definition of health expenditure and methodology, in consultation with peer and other stakeholders. This is an initiative by local researchers without external support, with an emphasis on putting various information systems into place. It involves two steps: the flow of funds from ultimate sources of finance to financing agencies; and the use of funds by financing agencies. • OBJECTIVES: • To analyze national health expenditure of Thailand from 1994 to 2005 by financing agent, health care function, and health provider, with the application of the OECD System of Health Accounts (OECD-SHA). Expenditure on health is defined by spending aiming at improvements of health of the population. • METHODS & DATA SOURCES: • Fourteen sources of health finance were aggregated into three main categories, namely government and non-government sources, and rest of the world. • Government health expenditure was collected from all concerned government organizations and institutes. • Secondary data analyses of a nationally representative household survey on household out-of-pocket payments for health in 1994 to 2005. • Health expenditure by the rest of the world was compiled from Thailand International Development Cooperation Agency (TICA) of the Ministry of Foreign Affairs. RESULTS: • In 2005, total health expenditure (THE) including capital formation in Thailand was 248 billion bahtat current prices, equivalent to US$ 8.0 billion. • The ratio of THE to GDP was 3.4 percent in 1994 and reached 4.1percent in 1997 in the year of the Asian Financial Crisis, and down to 3.6 percent in 2005. • In 1994, per capita THE at current prices was 2,160 baht (US$ 69.7) and increased rapidly to over 12 years to 3,974 baht (US$ 128.2) in 2005. • In 2005, around 78.5% of THE was used for purchasing personal medical services, of which curative and rehabilitative care services consumed 78.1% of THE. • The share of prevention and public health services was only 5% of THE in 2005. • In 2005, the share of public financing sources was 65 percent of THE, of which the central government was accountable for 52%, local government 3%, and the Social Health Insurance Scheme 8%. • The non-government sources shared 36% of THE in 2005, of which household out-of-pocket payments contributed the major share of 28%, and other private sectors represented 8% of THE. • An increasing share of public health financing sources has been observed, notably in 2001 to 2005. • Conclusions: • NHA can be used as a health financing diagnostic tool for evidence based policy making. • Main legacy of Thai NHA first phase in 1994 is a core group of inter-ministerial researchers who further developed the second phase for 1996-1998, the third phase for 1999-2001, and the fourth phase 2002-2005. Thai NHA has been produced by modifying OECD-SHA to suit the Thai context and policy utility as well as the advantage for international comparison. • NHA have limited use for health sector reform, and the reform requires multiple tools and multiple skills in addition to NHA. • Major enabling factors of Thai NHA are: national initiative among committed researchers which ensures ownership, continuous development, sustainability, and finally institutionalization of Thai NHA. For further information, contact Kanjana Tisayatikom (kanjana@ihpp.thaigov.net), and visit www.ihpp.thaigov.net. The Health System Research Institute (HSRI) and the Ministry of Public Health (MOPH) of Thailand funded this study.