Download
1 / 9
120 likes | 440 Views
RHEUMATOID VASCULITIS. Kamal Kolappa UNC Internal Medicine Morning Report 7.7.10. BACKGROUND. Rheumatoid Vasculitis (RV) is a rare complication of longstanding, severe Rheumatoid Arthritis (RA) Estimated incidence in 2-5% of RA patients 1

E N D
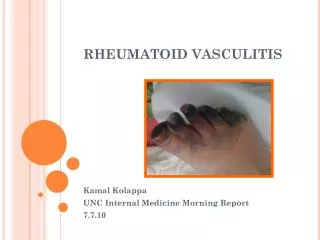
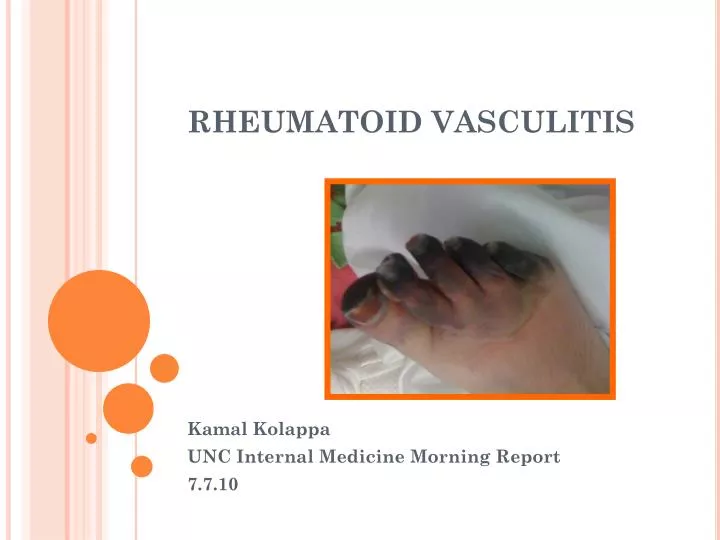
RHEUMATOID VASCULITIS Kamal Kolappa UNC Internal Medicine Morning Report 7.7.10
BACKGROUND • Rheumatoid Vasculitis (RV) is a rare complication of longstanding, severe Rheumatoid Arthritis (RA) • Estimated incidence in 2-5% of RA patients1 • Associated with chronic RA: Mean lag time 13.6 years between diagnosis of RA and onset of RV • Males are 2-4x more likely to develop RV than females • Characterized by Extra-Articular involvement of disease • Specifically the small and medium vessel arteries similar to polyarteritis nodosa • Correlated to high RF levels and low complement at onset of RV development; indicating uncontrolled RA disease as a risk factor2 • Anecdotal evidence that viral infections and drug reactions can precipitate RV occurrence in RA patients3 RV cutaneous ulcer
DISEASE MANIFESTATIONS • Cutaneous Manifestations secondary to vascular compromise (90% of RV patients evidence this)4 • Digital ischemia to fingers and toes • Cutaneous ulcers resulting from obstruction of superficial and medium vessels • Nail fold infarcts • Nerve Infarction (involves vasa vasorum) causing mononeuritis multiplex foot and wrist drop • Associated w/ neuropathy characterized by numbness, burning, pain that precedes muscle weakness, paralysis, and wasting • Ocular Scleritis • Non specific signs: Fever, Weight Loss Source: Up to Date
INVOLVEMENT OF LARGE ARTERIES CTA-Head +CTA Chest Of Ms. R • Classically, disease often limited to small and medium arteries; case reports of large artery involvement exist • Bowel6 • Renal • Brain (CVA’s) • Coronary Vasculitis (rare)5 • Focus back to Ms. R: • Extensive CVA w/o other leading cause (MCA distribution) • Hematuric evidence of possible Renal involvement • GG pulmonary opacities can be seen w/ pulmonary vasculitis • Large cecal perforation w/ bx proven vasculitic involvement
DIAGNOSIS OF RV Fibrinoid Necrosis in vessel wall Source: Up to Date • Evidence gathered from: • H&P: Suspect RV in any RA patient w/ fevers, weight loss, skin ulcerations, necrotic digits, or sx of sensory or motor nerve dysfxn • Labwork: specifically elevated RF7, low complement, elevated ESR, elevated Anti-CCP (citrullinated peptides) high odds ratio for possible RV in a person w/ h/o RA • Keep in Mind: No definitive Lab dx of RV • Imaging: Angiogram rarely useful as majority of vessels involved are medium (below image resolution); findings(segmental narrowing) are non-specific to RV • Full Thickness Skin Biopsy: As above, would show evidence of fibrinoid necrosis of vessels
DIFFERENTIAL DIAGNOSTIC CONSIDERATIONS • Cryoglobulinemia (Rx w/ Plex as opposed to immunosuppression Rx of RV)7 • Presents w/ palpable purpura, cutaneous ulcers, myalgias • Usually RF positive • Small vessel vasculitis of skin(purpura, pustules) usually not seen in RV as in Cryoglobulinemia • Polyartertis Nodosa (nearly indistinguishable from RV); key is clinical features, i.e. pt w/ strong hx of RA more likely has RV rather than PN • ANCA Vasculitides: Also RF positive • Wegener’s, Churg Strauss, Microscopic Polyangiitis • Vasculitis-like Syndromes • Thrombo-embolic phenomenon (cholesterol emboli) • Infectious Endocarditis (fever, skin lesions, active urine sediment)
TREATMENT OF RHEUMATOID VASCULITIS • Differs based on extent of involvement: Cutaneous vs. Systemic8 • Cutaneous Involvement • Isolated Nailfold Infarctions: secondary to low grade small vessel vasculitis symptomatic Rx, low risk of progression to systemic vasculitis • Leg ulcerations: Rx ~venous stasis, i.e. wet to moist saline dressings, compression bandages, hydrogel occlusive dressings; Higher assocation w/ systemic RV • Systemic RV • High Dose Glucocorticoids (1-3 days of Solumedrol 1gram/day) transition to PO Prednisone • Cytotoxic agent (e.g. Cyclophosphamide); Achieves disease remission; Alt: MTX, Azathoprione, TNF inhibitors
REFERENCES • 1. Voskuyl AE et al. Factors associated with the development of vasculitis in rheumatoid arthritis: results of a case-control study. Ann Rheum Dis. 1996; 55:190 • 2. Scott DG et al. Systemic Rheumatoid Arthritis: a clinical and laboratory study of 50 cases. Medicine(Baltimore) 1981; 60:288-290 • 3. Iyngkaran P et al. Rheumatoid vasculitis following influenza vaccination. Rheum. 2003; 42: 907-909 • 4. Sayah A et al. Rheumatoid Arthritis: A review of cutaneous manifestations. J Am Acad Dermatol. 2005; 53: 191-193 • 5. vanl Albada-Kuipers et al. Coronary arteritis complicating rheumatoid arthritis. Ann Rheum Dis. 1986; 45:963-968 • 6. Pagnoux C et al. Presentation and outcome of gastrointestinal involvement in systemic necrotizing vasculitides: analysis of 62 patients with polyarteritis nodosa, microscopic polyangiitis, wegener granulomatosis, churg-strauss syndrome, or rheumatoid-associated vasculitis. Medicine (Baltimore) 2005; 84:115-116 • 7. Geirsson AJ et al. Clinical and serological features of severe vasculitis in rheumatoid arthritis: A clinicopathologic and prognostic study of thirty-two patients. Arhtritis Rheum. 1995; 55:190-193 • 8. Abel T et al. Rheumatoid Vasculitis: effect of cyclophosphamide on the clinical course and levels of circulating immune complexes. Ann Internal Medicine. 1980; 93:407-408
APPRECIATE YOUR ATTENTION! Special Thanks to my Med U team: Eric Edwards, Andy Mcwilliams, Chris Sayed, Ross, Tim and Damon, Crystal, Eric Allman, and Paul Dombrower aka Master P