Download
1 / 60
600 likes | 620 Views
This toolkit supports implementing an Early Intervention System for effective treatment of musculoskeletal disorders, emphasizing the importance of timely intervention to restore functionality and prevent long-term disability. Learn about the business case development, influencers, and system change for Early Intervention. It includes principles such as assessment, standards of care, treat-to-target approach, and desired patient outcomes. Measurable targets are crucial to assessing system effectiveness and benefits.

E N D
Early Intervention Toolkit Toolkit to support the implementation of an Early Intervention System for the effective treatment of musculoskeletal disorders The toolkit
Benefits of EI Effectiveness of EI Implementing EI Developing the business case Influencers and system change Introduction Something about the importance of returning patients quickly to their original functionality enabling them to stay in work and be economically independent ( see text sent to Forster) Some evidential statement or something about economic benefit A brief explanation ( <100 words) of the EI approach to the treatment of musculoskeletal disorders Introduction Maybe a graph with explanatory text or something about healthcare system benefit Burden? need is to provide a solid evidence base for EI that shows the timings and can support a graph that will illustrate irreversibility over time. Home FfW Global Alliance
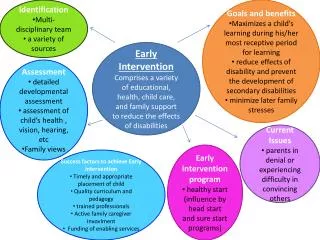
Introduction Benefits of EI Effectiveness of EI Implementing EI Developing the business case Influencers and system change Why is there a need for an Early Intervention System Benefits of Early Intervention What is Early Intervention Early intervention is ensuring the timing of any intervention is early enough to support the reversibility of disability at any age associated with any musculoskeletal disorder. Timingwill vary from problem to problem but the outcome is the same – restoring function and prevention of long term disability Initialising Event The initialising event is someone loosing functional capacity due to a musculoskeletal problem which is usually associated with pain. There may be work loss or difficulties with participating in other roles. Timing The timing of initial intervention is critical to ensure reversibility. There is no rule but evidence shows that the longer the initial intervention is delayed, then the more likely it is that the problem and associated disability is irreversible. Principles of Early Intervention Home 3 FfW Global Alliance
Introduction Benefits of EI Effectiveness of EI Implementing EI Developing the business case Influencers and system change What are the principles of Early Intervention Benefits of Early Intervention 1. Assessment EI needs early assessment by someone with appropriate competencies to characterise the problem, diagnose the cause if possible and develop and initiate a management plan. They need to recognise their limitations and if they are not able to diagnose or manage the problem appropriately, then they need to refer in a timely way to someone who can. 2. Standards of care There are established standards of care for the various MSK disorders which have chosen for being the most effective and most safe with treatment that can be initiated early. Rheumatoid Arthritis The modern management of rheumatoid arthritis exemplifies the importance of and gains from early intervention. Diagnostic criteria now predict the probability of persistent arthritis and disability to enable initiation of disease suppressing therapy as early as possible. 3. Treat to target Those delivering treatment to be trained in how to manage to ‘treat to target’ which involves setting a target, assessing disease activity and adjusting treatment accordingly. 4. Outcome The outcome of returning the patient to a functional level at which they are able to work and enjoy improved quality of life. Home 4 FfW Global Alliance
Introduction Benefits of EI Effectiveness of EI Implementing EI Developing the business case Influencers and system change How do we know we are there? Benefits of Early Intervention Measurable Targets The assessment of the effectiveness of an EI system requires measurable targets to be set, suggestions are: • reduction in temporary disability • reduction in permanent disability • percentage and timing of return to work • healthcare costs • social pension costs • out of work costs. Home 5 FfW Global Alliance
Introduction Benefits of EI Effectiveness of EI Implementing EI Developing the business case Influencers and system change Why is there a need for an Early Intervention System Benefits of Early Intervention • What is the impact of musculoskeletal disorders? Home 6 FfW Global Alliance
Introduction Benefits of EI Effectiveness of EI Implementing EI Developing the business case Influencers and system change What is Early Intervention in practice, when is Early Intervention most effective and what can it offer Effectiveness of Early Intervention • Examples of best practice using template Home 7 FfW Global Alliance
Introduction Benefits of EI Effectiveness of EI Implementing EI Developing the business case Influencers and system change What is Early Intervention in practice, when is Early Intervention most effective and what can it offer Effectiveness of Early Intervention • Evidence library from systematic review of literature Home 8 FfW Global Alliance
Introduction Benefits of EI Effectiveness of EI Implementing EI Developing the business case Influencers and system change How to implement Early Intervention Implementing Early Intervention Models of care based on EI Audit tool including benchmarks of best practice Barriers and facilitators Indicators for health and social care system readiness for MSK EI Home 9 FfW Global Alliance
How to implement Early Intervention • Models of care based on EI • Points to consider in developing a model of care to deliver MSK EI • Take key principles from literature and case studies • Use Framework to Evaluate MSK Models of Care • Need for explicit standards of care - EUMUSC
How to implement Early Intervention • Models of care based on EI • It was suggested that the approach should be the development of an “ideal” model of care for EI rather than using specific models of care. • To achieve this a literature search will be carried out prior to further discussion with the project group and consensus will be achieved using Nominal Group Technique (NGT). • It was agreed that the models of care would need to be disease based. • The discussion also considered the need to develop models of care on a health system basis; it is understood that recent work in Australia by Prof Andrew Briggs used the concept of health system readiness. It was suggested that the project group should develop an ideal model and then identify the key elements that may differ between health systems and the adjustments that would be required to embed the model in specific health systems.
Models of Care What is a Model of Care? • A Model of Care (MoC) is a principle-based guide that describes best practice care for particular health conditions or populations. The focus is on person‑centred care and consideration of applicability in local settings. A MoC is not an operational plan for a health service or a clinical practice guideline. Who uses Models of Care? • MoCs have cross-sector and multi-stakeholder relevance. Policy makers, health administrators and managers, service delivery organisations, clinicians, researchers, funders, advocacy organisationsand consumers use MoCs to inform best practiceplanningand delivery of health services. Purpose of the Framework • To develop a comprehensive evaluation framework to assess the readiness for implementation and success after implementation of Early Intervention MSK MoCs. • The Framework provides principle-based guidance on evaluating these important areas. Particular emphasis is placed on ensuring the Framework is applicable across a diverse range of environments and contexts.
Model of Care • A Model of Care (MoC) is a person-centredand principle-based guide, usually presented as a document that describes: • evidence-informed, best practice care for particular health conditions (in this case, musculoskeletal conditions) • whatcare should be provided • howit should be delivered at a regional or national level
Models of Care for Early Intervention in Common MSK Conditions • Key principles • Early access to healthcare – case identification of someone with a disabling MSD and referral • Protocoled management – 3 levels – diagnostic / therapeutic • Outcomes focused function and on participation, especially work • Exit from programme – recovered or non-recoverable • Every contact counts • Rapid triage to appropriate level of care • Plan return into work • Appropriate resources • Health system that offers timely access to appropriate care • Capacity • Competent workforce • Investigations • Interventions • Rehabilitation • Pharmacological • Surgical
Protocolled management based on three levels of growing complexity Level 1. Clinical Management by the Rheumatologist (Expert/Specialist) • Diagnosis based on clinical criteria. • Rule out warning signs (APPENDIX B). • Pharmacological treatment of pain, inflammation, anxiety and depression. • Arthrocentesisand intra/periarticular injections. • Avoid unnecessary tests and interconsultation. • Provide the patient with frequent check-ups. • The time at this level depends on the pathology, but less than 8 weeks. • The vast majority of patients recover at this level due close monitoring with frequent check-ups by same physician, information on pathology and treatment, early and intensive treatment with correct use of painkillers (fixed schedules and appropriate pharmacological strength), promotion of early mobilization and self-movement, and patient education.
Protocolled management based on three levels of growing complexity Level 2. Limited and selective diagnostic tests are added at the first level • Rule out warning signs. • Identification of serious or intercurrent diseases. • Identification of confounding factors: Psychological, Family, Social, Work and Occupational. • Limited and selective diagnostic tests are recommended to suit each situation (X-rays, EMG, CT/MRI). • Cell Blood Count (CBC), Biochemical, ESR and high sensitive CRP to rule out serious disease. • Opportune modifications to the pharmacological treatment. • Keep educating the patient. • The time at this level depends on the pathology, but less than 10 weeks
Protocolled management based on three levels of growing complexity Level 3. In addition to the previous levels there is the care provided by other professionals, including complex therapeutic and diagnostic evaluations. It would include, inter alia: • Formal rehabilitation. • Evaluation by other specialists. • Musculoskeletal surgery. • Neurosurgery. • Pain unit. • Invasive techniques. • Cognitive behavioural therapies.
Models of Care for Early Intervention in Common MSK Conditions • Low back pain • Neck pain • Upper limb pain • Lower limb pain • Muscle pain • Carpal tunnel syndrome • Internal knee disorder • Peripheral osteoarthritis • Inflammatory joint diseases
Patient Education Diagnosis, Treatment and Prognosis • Always provide a diagnosis upon the first visit. • Positively explain whether it is a very frequent diagnosis and the vast majority of people improve within a short space of time. • Promote the trust and active collaboration of the patient, explaining that treatment will be started soonest and the success of the treatment depends on the patient taking the medication properly and following the rest of the guidance. • Ensure that we will carry out a check-up in the near future and that if evolution is not in the manner desired, we will use every measure required.
Patient Education Avoid the fear of pain • Explain to the patient that pain does not have to be a synonym for major damage. • Explain that we will provide him with the medication he requires, that his pain will get better and that it will take a while for it to go away totally. • Stress that what matters is whether you can lead a normal life, even if there is a light and moderate pain. • Explain that functionality improvement is witnessed first, followed by improvement in pain.
Patient Education Promote general and local mobilisation • Work on “fear of movement”, in other words, that the problem will get worse with movement. • Totally discourage resting in bed. • Promote walking and progressive aerobic exercises. • Insist on carrying out specific exercises, even if they are uncomfortable.
Patient Education Promote an early return to work • Explaining that work is good for health. • Reassure the patient that it is possible to go back to work without feeling 100%. • Help the patientovercomefear of going back towork, explainingthata comprehensive monitoring willbedoneandif the patient is unabletocomewithwork, a sick notewillbeissuedagain.
Patient Education Promote moderate physical activity (APPENDIX E) • Very important in low back pain, neck pain, fibromyalgia… • Moderate aerobic exercises: walking quickly, swimming, dancing, cycling…. • This is measured by the pulse according to age. Between 90-110 ppm. A heart rate monitor may be used. • Equivalent to walking rapidly. • 30-45´ vital, five days a week.
Patient Education Teach and indicate recommended and specific exercises (APPENDIX E): • Axial exercises • Extensors and flexors: key to neck pain and low back pain. • Hand out leaflet • Regional and local exercises • Important with joint and tendon situations. • Joint: isometric, no load, with load. • Tendons: stretching and strengthening.
Patient Education Provide self-management instructions • Traditional therapies (managing the cold, heat, self-massage). • Ergonomic care (postural hygiene, joint overload protection).
Pharmacological Management • Take advantage of level II analgesia • Make use of injections in peripheral affectations • Guarantee therapeutic compliance • Fixed treatments with a timetable. • Carry out frequent check-ups. • Maintain treatment in the first stages of work reinsertion.
Return to work • Enable the patient to return to work in a calm and confident manner and feel he has been supported in the process, with the use of the following simple measures: • planning discharge in a manner in which the patient resumes his activities in the middle of the working week, being given one or two days of rest 72 - 96 hours after reintegration • maintaining pharmacological treatment for the first week, with a gradual reduction in the dose while adapting to the new situation • Guaranteeing a scheduled medical visit to assess clinical and functional progress.
Evaluation (1) • It is important to conduct an assessment of the results achieved by the programmein order to confirm the efficacy uphold the collaborative effort. • Working population covered by the programme: calculated on a specific population area: • Number (no.) of employees who have the TWD-MSDs programmeat their disposal. • Percentage (%) of employees who have the TWD-MSDs programmeat their disposal. • Programme activity: • Number (no.) of TWD-MSDs processes dealt with. • Percentage (%) of TWD-MSDs Processes of a given health area dealt with in the TWD-MSD Programme.
Evaluation (2) • Programme quality: evaluation of two main characteristics - early referral and intensity of the follow-up: • Percentage (%) of TWD-MSDs episodes dealt with in the first week of sick leave. • Ratio of check-ups/new visits. • Efficacy: • Variables could include: • Total no. of TWD-MSDs • Mean duration of TWD-MSDs • Total days of TWD-MSDs • Number of patients with PWD • Estimated saving in payment of compensations • Comparator groups which allows an evaluation of the efficacy of a TWD-MSDs Programme could include: • Historic control group from the same health area • Parallel control group from another area in the same Region • The whole Region • The other Regions
Evaluation (3) • Results of Social Security Expenditure Rationalisation • take into account indicators that relate to expenditure and also those of epidemiological nature. • Cost/affiliate/month - use lengthy time periods in asprogrammeeffectiveness increases over time and quarterly, half-yearly, annual and biannual periods can be compared. • Other Indicators • Incidence. TWD processes commenced/1000 affiliates • Prevalence. TWD processes ongoing/1000 affiliates • TWD days/affiliate
Red Flags Warning signs of serious disease with symptoms of pain in any location: • Fever • Weight loss • Night-time pain • Adenopathies • Prior trauma • Tumoralpathology or prior serious disease • Drug abuse • Use of immunosuppresor treatments Warning signs of serious disease with symptoms of axial pain: • General signs of a serious disease • Loss of strength or Paralysis at extremities • Sphincter Incontinence (lower backpain) • Saddle anaesthesia (lower back pain) • Absence of peripheral pulses • Change in coloration and temperature at extremities • Constant, progressive symptomatology Warning signs of serious disease with symptoms of pain at extremities: • General signs of a serious disease • Sensitive or motor Neurological • Symptoms • Muscle atrophy • Absence of peripheral pulses • Change in coloration and • temperature at extremities • Ungealinfarcts
Yellow Flags • Psychiatric Disease • Occupational, social or family conflicts (problems) • Unemployed • Occupational (work) etiology of the present pathology
How to implement Early Intervention • Audit tool including benchmarks of best practice • Agree what to audit for EI – what quality indicators – EUMUSC, MoC Framework
How to implement Early Intervention • Audit tool including benchmarks of best practice • 1) process measures based on how quickly the patient was seen • 2) work measure based on how quickly the patient was able to return to work • 3) journey measure based on patient reported outcome measures • 4) disease measures for those diseases with recognised measures • 5) healthcare setting/system settings • I wouldn’t restrict the discussion on how quickly the patient was able to return to work, as there are a lot of methodological concerns with the outcome parameter RTW. Maybe we can include aspects such as workability as well
Optimising development for sustainableimplementation. • A range of system, organisationaland provider factors can be a barrier to achieving sustainable implementation of MoCs. • There is merit, therefore, in optimisingthe ‘readiness’ of a MoCfor implementation by considering what might be an ideal MoCdevelopment process and one, which will also enable sustainable implementation.
Evaluating outcomes of Models of Care • Evaluation of MoCs is critical as a step to inform and drive health reform and share evaluation experiences between countries. • Identifying indicators of success and guiding how to measure these indicators is important for: • local stakeholders such as governments • sharing outcomes • undertaking benchmarking internationally and across jurisdictions.
READINESS STREAM • This stream is relevant to developers at a national or regional level. • This stream outlines: • what should be included in a regional or national MoC • how it should be presented and the process of development. Key domains • Structure and components of a MoC document • Engagement and consultation • Promoting best practice by describing what care and how to deliver it • Consumer centric
Structure and components of a MoCdocument • A clear outline • A data-driven case for change • Define target population / priority group • Cost-effectiveness data
Engagement and Consultation • Important stakeholders • What to ask and explore • Seeking endorsement • Identifying and supporting local champions
Promoting best practice by describing what care and how to deliver it • Align contemporary standards • Identify required behavioural changes • Utilise different service delivery modes • Specify communication and referral pathways
Consumer centric • Practical, user-friendly recommendations • Partnership-based service delivery and funding
INITIATING IMPLEMENTATION STREAM • This stream describes how to approach implementation after a MoChas been developed. It provides guidance on what to consider for optimising implementation success and how to develop an implementation plan. This stream is relevant to those tasked with implementation of a MoC, usually at a local or regional level. KEY DOMAIN • Optimising implementation and evaluation process
Optimising implementation and evaluation process • Asses system readiness • Linking to local resources • Identifying likely workforce requirements • Building a comprehensive implementation plan • Formative evaluation of MoC components • Establishing a user reference group
SUCCESS STREAM • This stream considers how to approach evaluation, including both formative evaluation and impact evaluation that includes consumer and system-relevant outcomes. This stream is relevant to those asked with monitoring the outcomes of a MoC, usually at a local or regional level Key domains • Continuous improvement processes • Key performance indicators • Engagement and participation • Uptake and integration
Continuous improvement process • Pragmatic evaluations over time • Quality assurance and troubleshooting mechanisms • Data collection for key performance indicators • Promoting research priorities
Key performance indicators • Consumer relevant outcomes • Service delivery partnerships and pathways • Cost-effectiveness • Stakeholder behaviour changes
Engagement and participation • Awareness and knowledge of the MoC • Reach to target population • Satisfaction with process and programmes