Download

1 / 0
0 likes | 423 Views
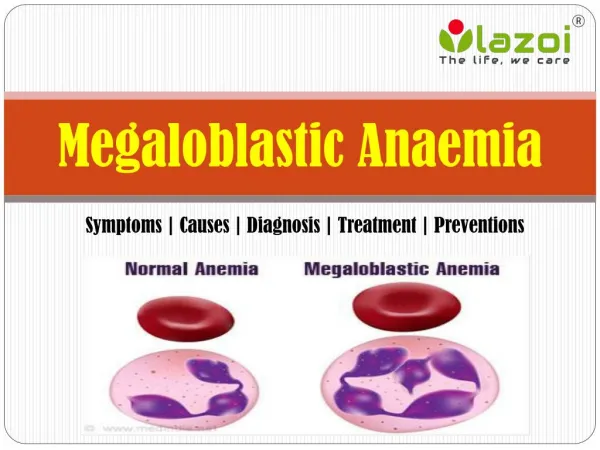
An intelligent approach to the diagnosis and treatment of Anaemia. Prof. Aziz-ur-Rehman. Introduction. Very common problem Subtle or no symptoms, usually incidental finding Various causes; ID is the commonest Simple iron replacement is not the solution Investigate before starting treatment.

E N D