Download
1 / 1
10 likes | 117 Views
Purpose :

E N D
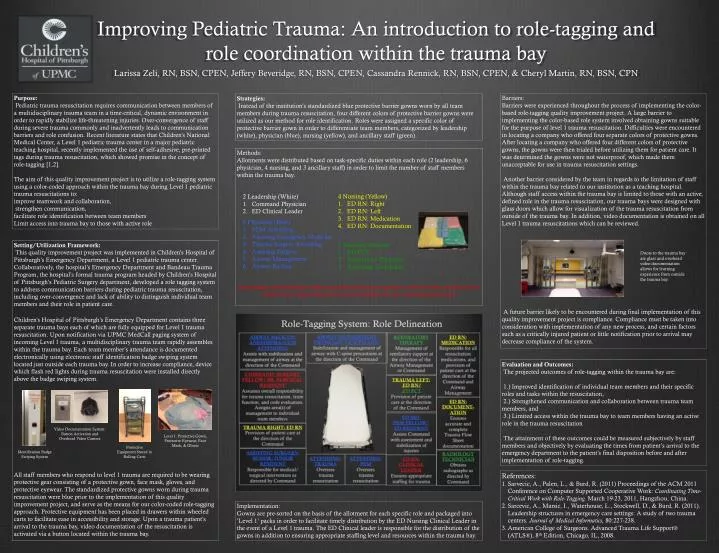
Purpose: Pediatric trauma resuscitation requires communication between members of a multidisciplinary trauma team in a time-critical, dynamic environment in order to rapidly stabilize life-threatening injuries. Over-convergence of staff during severe trauma commonly and inadvertently leads to communication barriers and role confusion. Recent literature states that Children’s National Medical Center, a Level 1 pediatric trauma center in a major pediatric teaching hospital, recently implemented the use of self-adhesive, pre-printed tags during trauma resuscitation, which showed promise in the concept of role-tagging [1,2]. The aim of this quality improvement project is to utilize a role-tagging system using a color-coded approach within the trauma bay during Level 1 pediatric trauma resuscitations to: improve teamwork and collaboration, strengthen communication, facilitate role identification between team members Limit access into trauma bay to those with active role Barriers: Barriers were experienced throughout the process of implementing the color-based role-tagging quality improvement project. A large barrier to implementing the color-based role system involved obtaining gowns suitable for the purpose of level 1 trauma resuscitation. Difficulties were encountered in locating a company who offered four separate colors of protective gowns. After locating a company who offered four different colors of protective gowns, the gowns were then trialed before utilizing them for patient care. It was determined the gowns were not waterproof, which made them unacceptable for use in trauma resuscitation settings. Another barrier considered by the team in regards to the limitation of staff within the trauma bay related to our institution as a teaching hospital. Although staff access within the trauma bay is limited to those with an active, defined role in the trauma resuscitation, our trauma bays were designed with glass doors which allow for visualization of the trauma resuscitation from outside of the trauma bay. In addition, video documentation is obtained on all Level 1 trauma resuscitations which can be reviewed. A future barrier likely to be encountered during final implementation of this quality improvement project is compliance. Compliance must be taken into consideration with implementation of any new process, and certain factors such as a critically injured patient or little notification prior to arrival may decrease compliance of the system. Strategies: Instead of the institution’s standardized blue protective barrier gowns worn by all team members during trauma resuscitation, four different colors of protective barrier gowns were utilized as our method for role identification. Roles were assigned a specific color of protective barrier gown in order to differentiate team members, categorized by leadership (white), physician (blue), nursing (yellow), and ancillary staff (green). Methods: Allotments were distributed based on task-specific duties within each role (2 leadership, 6 physician, 4 nursing, and 3 ancillary staff) in order to limit the number of staff members within the trauma bay. 4 Nursing (Yellow) ED RN: Right ED RN: Left ED RN: Medication ED RN: Documentation 2 Leadership (White) Command Physician ED Clinical Leader • 6 Physician (Blue) • PEM Attending • Assisting Emergency Medicine • Trauma Surgery Attending • Assisting Surgery • Airway Management • Airway Backup 3 Ancillary (Green) ED PCT Respiratory Therapist Radiology Technician Setting/Utilization Framework: This quality improvement project was implemented in Children’s Hospital of Pittsburgh’s Emergency Department, a Level 1 pediatric trauma center. Collaboratively, the hospital’s Emergency Department and Bandeau Trauma Program, the hospital’s formal trauma program headed by Children’s Hospital of Pittsburgh’s Pediatric Surgery department, developed a role tagging system to address communication barriers during pediatric trauma resuscitation, including over-convergence and lack of ability to distinguish individual team members and their role in patient care. Children’s Hospital of Pittsburgh’s Emergency Department contains three separate trauma bays each of which are fully equipped for Level 1 trauma resuscitation. Upon notification via UPMC MedCall paging system of incoming Level 1 trauma, a multidisciplinary trauma team rapidly assembles within the trauma bay. Each team member’s attendance is documented electronically using electronic staff identification badge swiping system located just outside each trauma bay. In order to increase compliance, device which flash red lights during trauma resuscitation were installed directly above the badge swiping system. All staff members who respond to level 1 trauma are required to be wearing protective gear consisting of a protective gown, face mask, gloves, and protective eyewear. The standardized protective gowns worn during trauma resuscitation were blue prior to the implementation of this quality improvement project, and serve as the means for our color-coded role-tagging approach. Protective equipment has been placed in drawers within wheeled carts to facilitate ease in accessibility and storage. Upon a trauma patient’s arrival to the trauma bay, video documentation of the resuscitation is activated via a button located within the trauma bay. Doors to the trauma bay are glass and overhead video documentation allows for learning experience from outside the trauma bay. Improving Pediatric Trauma: An introduction to role-tagging and role coordination within the trauma bay Larissa Zeli, RN, BSN, CPEN, Jeffery Beveridge, RN, BSN, CPEN, Cassandra Rennick, RN, BSN, CPEN, & Cheryl Martin, RN, BSN, CPN Responding staff members without specified roles are required to observe from outside of the trauma bay, unless directed to assist at bedside by the Command physician Evaluation and Outcomes: The projected outcomes of role-tagging within the trauma bay are: 1.) Improved identification of individual team members and their specific roles and tasks within the resuscitation, 2.) Strengthened communication and collaboration between trauma team members, and 3.) Limited access within the trauma bay to team members having an active role in the trauma resuscitation The attainment of these outcomes could be measured subjectively by staff members and objectively by evaluating the times from patient’s arrival to the emergency department to the patient’s final disposition before and after implementation of role-tagging. Video Documentation System: Button Activation and Overhead Video Camera Level 1: Protective Gown, Protective Eyewear, Face Mask, & Gloves Protective Equipment Stored in Rolling Carts Identification Badge Swiping System • References: • Sarvecic, A., Palen, L., & Burd, R. (2011) Proceedings of the ACM 2011 Conference on Computer Supported Cooperative Work: Coordinating Time-Critical Work with Role-Tagging. March 19-23, 2011, Hangzhou, China. • Sarcevic, A., Marsic, I., Waterhouse, L., Stockwell, D., & Burd, R. (2011). Leadership structures in emergency care settings: A study of two trauma centers. Journal of Medical Informatics, 80:227-238. • American College of Surgeons. Advanced Trauma Life Support® (ATLS®), 8th Edition, Chicago, IL, 2008. Implementation: Gowns are pre-sorted on the basis of the allotment for each specific role and packaged into ’Level 1’ packs in order to facilitate timely distribution by the ED Nursing Clinical Leader in the event of a Level 1 trauma. The ED Clinical leader is responsible for the distribution of the gowns in addition to ensuring appropriate staffing level and resources within the trauma bay.