Download
1 / 25
250 likes | 374 Views
Discharge Planning and Transitions of Care: Where are they going and why?. Opening the Black Box. Exercise.

E N D
Discharge Planning and Transitions of Care:Where are they going and why? Opening the Black Box
Exercise • You admit an 80 yr old woman in transfer from a outside facility. There is no hospital summary, only loose papers and a cover sheet listing hospital admission date and meds (unclear if admission or transfer meds). Her family is unavailable. • She is delirious, hypertensive, and severely impacted • The last labs sent with her are from 3 days old; Hgb was 7.8 and creat 2.2. • You call the hospital and the floor RN says the pt was discharged on the previous shift and she knows nothing about the patient.
Exercise • You admit an 80 yr old woman in transfer from a outside facility. There is no hospital summary, only loose papers and a cover sheet listing hospital admission date and meds (unclear if admission or transfer meds). Her family is unavailable. • She is delirious, hypertensive, and severely impacted • The last labs sent with her are from 3 days old; Hgb was 7.8 and creat 2.2. • You call the hospital and the floor RN says the pt was discharged on the previous shift and she knows nothing about the patient. This is a routine skilled nursing facility admission
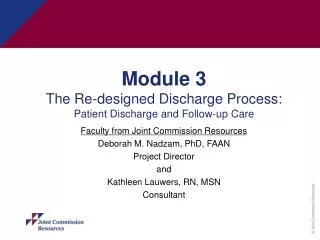
A Life Birth Marriage Retirement Age 50 Death Episodes of Serious Illness Courtesy Peter Boling, MD
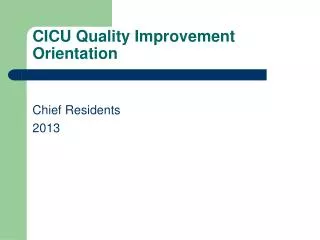
Scope of the Problem:Hospital Admission = First of Multiple care transitions 18 days in hospital,35days in NH, 135 days of homecare, 312days at home Hospital: MI, CHF Hospital: CHF Hospital: A-fib, Stroke 4 days 8 days 6 days 35 45 28 62 Home Health Episodes Nursing Home Stay Courtesy Peter Boling, MD
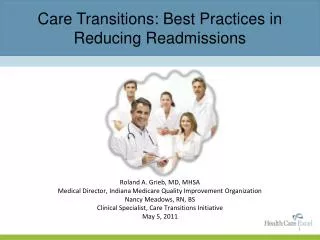
Discharge from Hospital to Other Institutions increases with Age AHRQ HCUPnet http://www.ahrq.gov/data/hcup/factbk1/10shel.htm
Discharge Planning • All team members should participate − begin early in hospital course • Site of care after D/C should be warranted by patient’s needs • MD: Assess medical care needs, provide D/C summary and orders, do med reconciliation
TransitionPlanning • All team members should participate − begin early in hospital course • Site of care after D/C should be warranted by patient’s needs • MD: Assess medical care needs, provide D/C summary and orders, do med reconciliation
Where can patients go after hospitalization? • Home • Home with services • Inpatient Rehab • Chronic Care Hospital • Skilled Nursing Facility (SNF) • Hospice
Who Pays For What? Medicaid • to qualify, income and assets must be below state eligibility levels • $880/$2,000 indiv, $1090/$3,000 couple • $8,000 set aside in burial contract Medicare • Age > 65 • Part A – hospital, SNF, hospice; no premium • Part B – MD visits, outpatient expenses, home health care; pay premium • Part D – medications
Many possible options for “Home” • House, apartment; alone, with spouse and/or other family • Senior Housing • Continuing Care Retirement Community (CCRCs) • Assisted Living Facilities, Residential Care Facilities, Board and Care • Nursing Home
Home Care The provision of diagnostic, therapeutic or support services to the patient in the home for the purpose of restoring and maintaining his or her maximal level of comfort, function, and health. AMA Council on Scientific Affairs, JAMA 1990; 263 1241-1244 Levine SA et al. JAMA 2003; 290:1203-1207.
Medicare Services in Home Care • Part A (hospital) • Visiting nurse • HHA • SW • Mental Heath • Dietician • OT/PT/ST • Part B (20% co-pay) • MD Home Visit • Durable medical equipment • Diagnostics
Medicare: “Skilled” Home Care via Certified Home Health Agency • A physician can refer any patient with an acute skilled need to a home care agency • Nursing care • Monitoring of vital signs, cor/pulm status • Wound care • DM monitoring and education • Medication management • PT and OT • Speech therapy
Durable Medical Equipment • Covered by Medicare (mostly) • Specific Requirements Courtesy of Jeremy Boal, MD
Non Durable Equipment • Adult Incontinence Pads • Chux • Booties • Gloves • Wound care supplies • Not covered by Medicare • May be covered by Medicaid
What Medicare Doesn’t Pay For • Homemaker • All bathroom equipment • Transportation • Personal or supportive long-term care
Skilled Nursing and Rehab in Nursing Homes • Medicare pays if 3 day/night in hospital and 24 hr skilled nursing care needed • Duration of coverage depends on types and number of skilled needs • Integrates features of acute care/rehab • Interdisciplinary staffing • Nursing: RN, LPN, CNA, wound care • Therapies: PT/OT/ST, nutrition, SW, etc • Medical: MD, PAs, NPs • Other clinical: dental, podiatry, vision, psych, psychology, clinical pharmacist
Ancillary Services • Phlebotomy/Laboratory • Radiology • EKG • Venous dopplers • IVs: peripheral, PICC, etc • No Dobhoffs or Central Lines
Acute Inpatient Rehab • Needs and can tolerate intensive PT/OT (3 hrs/day) • Medically unstable for SNF • Needs frequent MD evaluation (> q1-2 wk) • Rising Cr, dropping Hgb • Meds will need adjustment in < 24-48 hr (eg, BP meds, diuretics) • Needs telemetry, daily/STAT labs
4 Core Elements of Transition Information and Communication • Medical needs • Summary of admitting problems and course • Active Problem list • Recent and important pending labs • Reconciled Medication List (incl admit meds and all changes) and allergies • Advance directives: DPOA-HC, preferences, goals • Functional support (ADL, IADL) • Disposition: where from and where next • Functional status: baseline and present • Social support and contact info • Nursing needs: monitoring, wounds • Rehabilitative needs: PT, OT