Download

1 / 63
640 likes | 677 Views
Learn about Leishmaniasis caused by protozoan parasites, its global epidemiology, vector transmission, and clinical manifestations including cutaneous and visceral forms.

E N D
Leishmaniasis (Kala azar and other forms) Nedim Çakır Neu-med.
Etiology • A protozoan disease caused by Trypanasomidae family • Twenty of total 30 species may cause diseases in mamalians • Last classification CAKIR: LEISHMANIASIS 2014-2015 2
Etiology-2 • Human cutaneous – mucucutaneous leishmaniasis : • L. braziliensis complex : L. braziliensis, L. panamensis/ L. guyanensis, L. shawi and L. Peruviana • L. mexicana complex: L. mexicana, L. amazonensis, L. Venezuelensis, L. lainsoni, L. Naifi ve L. lindenbergi. • L. tropica complex: L. tropica, L. anmdL. aethiopica, • Human visceral leishmaniasis agents: • Leishmania donovani (includ. L. archibaldi’yi) and L. infantum/ L. chagasi CAKIR: LEISHMANIASIS 2014-2015 3
Etiology-epidemiology • Old World: L. İnfantum • New World: L. chagasi • Bu iki son etken eskiden ayrı türler gibi kabul edilmişse de yapılan analizlerde bunların tek tür oldukları anlaşılmıştır • L infantum may cause also cutaneous form without systemic infection CAKIR: LEISHMANIASIS 2014-2015 4
Global epidemiology-1 • All over the world except Australia, Oceania, Pasific Isld.s • Hyperendemic areas: Afghanistan, Brasil, Sudan CAKIR: LEISHMANIASIS 2014-2015
Global epidemiology-2 Most of patients (90 %) • Visceral form: Bangladesh, Basil,India, Nepal and Sudan • Muco-cutaneous form: Bolivia, Brasil, and Peru • Cutaneous form : Afghanistan, Brasil, Iran, Peru, Saudi Arabia, Syria • Mainly undeveloped countries and areas • In 33/88 countries unreported/ CAKIR: LEISHMANIASIS 2014-2015
Global epidemiology-3 • Totally 350 million patients • 350 million people are at risk worldwide (in six countries: Bangladesh, Ethiopia, Brazil, India, South Sudan and Sudan) • 12 Milionnew cases every year • Equal in rural and urban areas • HIV co-infections are at higher severity risk CAKIR: LEISHMANIASIS 2014-2015
Transmission: • Via biological vectors: • Phlebotomus and • Lutzomyia, • Each leishmania species adoptto and can survive in few phlebotomus species • Only female phlebotomus are responsible from transmission • Effect of seasonal conditions: • Dry and windless seasons, • Higher humidity • Time:Dawn and evening hours • Daytime: If they were disturbed in their hollow CAKIR: LEISHMANIASIS 2014-2015 8
Vector • Female phlebotomiade members • Old world Phlebotomus Phlebotomus papatasi • New world Lutzomyia ♀ ♀ ♂ Lutzomyia mignoei Vector of L infantum CAKIR: LEISHMANIASIS 2014-2015
Transmission: • Natural habitat: • Daytime • Animal shelters • Tree hollows, • evlerin görece serin ve nemli yerleri • Nighttime • Lighting attracts • Mechanical vectors: • Ticks(Dermacentor variabilis and Rhipicephalus sanguineus), dog’s flea • Dother transmission routes: • Asymptomatic individuals, • Blood transfusions, • Transplacental route (Vertical transmissions): Dogs, rats,and humans, Dog’s urine, tear, saliva or other secrets like semen, • Dogfights or dog lickings may responsible to transmissions l CAKIR: LEISHMANIASIS 2014-2015 10
L infantum amastigotes in dog macrophages CAKIR: LEISHMANIASIS 2014-2015 11
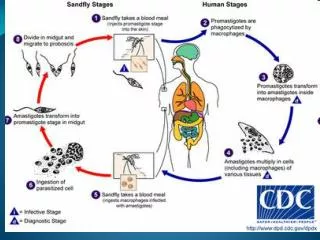
Lifecycle of leishmaniasis CAKIR: LEISHMANIASIS 2014-2015 12
Life cycle of Leishmania-1 Two stages have been detected: • Promastigot stage: Flagellated.. In vectors gut • Amastigot stage: Seen in mammary cells as intracellulary form • Only female Phlebotoms can transmit promastigots by biting • Parasites engulfed by macrophages and dendritic cells in dermis CAKIR: LEISHMANIASIS 2014-2015 13
Life cycle of Leishmania-2 • Losts flagels within dendritic cells amastigot form • Engulfed parasite remains alive in phagolysosomes • İnvades lymphatic and vasculary tissues • İnvades mocytic anda macrophages in RES Bone marrow infiltration, heptomegaly, splenomegaly, lymphadenopathy, CAKIR: LEISHMANIASIS 2014-2015 14
Epidemiology of VL • L. infantum infections Mainly immune deficient patients and infants • L. Donovani All ages • Global epidemiology: Yearly • 500,000 new cases • 50,000 death • The second most important parasitic infection after malaria CAKIR: LEISHMANIASIS 2014-2015 15
Epidemiolgy ofL donovani, L infantumand L chagasi CAKIR: LEISHMANIASIS 2014-2015 16
Layşmanyoz klinik epidemiyolojisi CAKIR: LEISHMANIASIS 2014-2015 17
Clinical picture of Leishmaniasis CAKIR: LEISHMANIASIS 2014-2015
Layşmanyoz klinik tipleri • Cutaneous (Dermal leishmaniasis) (CL) • Localised cutaneous leishmaniasis (Oriental sore, Şark çıbanı) • Diffuse cutaneous leishmaniasis • Leishmaniasis residivans • Post kala azar dermal eishmaiasis (PKDL) • Mucocutaneous leishmaniasis (MCL) • Visceral leishmaiasis (Kala azar) (VL) • Viscerotropic leishmaiasis (VTL) CAKIR: LEISHMANIASIS 2014-2015 20
Cutaneous leishmaniasis • Dermal involvement • Single lesion multiple (Dozens) • Appearance of lesion: Depend upon the clinical types • Ulcers, • Nodules, • Düz plaklar veya • hyperkeratotic wart-like lesions CAKIR: LEISHMANIASIS 2014-2015
CL (Şark çıbanı) • Initial lesions: Papule at phlebotomus bite site • Lesions can remain antry-sites (Not as a rule) • Secondary lesions: • Lymphatic involvement • Skin and mucosal involvement • Secondary lymphanenopathy • Characteristics of cutaneous lesions: • Painless • Secondary lesions can be painful • Generally painful if auricular lesions • Mainly no subcutaneous incolvement • Outcome: • Spontaneous recovery depend upon clinical pictures • Few monthsfew years • Some forms remain in permanent scars (oriental sore) • Severe clinical forms: • HIV co-infections • Other immune deficiency patients CAKIR: LEISHMANIASIS 2014-2015
Cutaneous leishmaniasis (Oriental sore: Şark çıbanı) CAKIR: LEISHMANIASIS 2014-2015
Orld World cutaneous leishmaniasis: ORİENTAL SORE ŞARK ÇIBANI CAKIR: LEISHMANIASIS 2014-2015
CL: Disseminated form • Fairly seldom • Seen in : • L. amazonensis infections • More frequent in New World • Esatern hemisphere: • in HIV coinfections • İmmune deficiency CAKIR: LEISHMANIASIS 2014-2015
In L aethiopica/mexicana komplex infections Chronic, prgressive, anerjiic variant Nodules cannot turn ulcerative forms Invades skin. Deep tissues invasion also Resistant to treatment Diffuse cutaneous leishmaniasis(DCL): CAKIR: LEISHMANIASIS 2014-2015
L tropica and L braziliensis After recovery of primary lesions As satellite lesions around recovered cutaneous form No spontaneous recovery. Leishmaniasis rezidivans (Lupoid leishmaniasis) (LR): CAKIR: LEISHMANIASIS 2014-2015
Mucocutaneous llwishmaniasis (Espundia) (MCL): • Most patient from Latin America • Agent(s): • L. braziliensis braziliensis (generally) • L. panamensis/ L. Guyanensis (seldomly) • Due to extension of local skin disease into the mucosal tissue via • direct extension, • bloodstream or • lymphatics. • Appearance of syptoms: • Few years after healing of CL • Sometimes together Epistaxis • Initial lesions: • Hyperemia around nostrils CAKIR: LEISHMANIASIS 2014-2015
Mucocutaneous llwishmaniasis (Espundia) (MCL)(Cont’d) • Clinical pictures: • Inflamation Tissue destruction • İnvades to nasal septa • Pharyngeal and/or laryngeal invasion • Septal perforation • Malformations (Papağan gagası, deve burnu görünümü) • Obstruction of pharynx and/or larynx • Rarely invasion of genitalia • No spontaneous healing, Patients need treatment CAKIR: LEISHMANIASIS 2014-2015
Visceral Leishmaniasis (VL)Kala azarDum Dum fever CAKIR: LEISHMANIASIS 2014-2015
Clinical signs: General • Incubation period: 2-6 mo. • Persistant systemic signs: Fever, malaise, fatigue, loss of apetite • Organomegaly: • Hepatomegaly • Splenomegaly • Other RES involvement: lymphatic CAKIR: LEISHMANIASIS 2014-2015 32
Other caharacteristics of VL • Agent(s):Leishmania donovani complex • May fatal if not treat • Systemic symptoms • Leishmania infantum: Common in TRNC and Middle East Europe- NorthAfrica, and Latin Americada CAKIR: LEISHMANIASIS 2014-2015 33
Other caharacteristics of VL(Cont’d) Clinical types of VL • Zoonotic VL (ZVL): • Reservoir: Animals • Vector: Phlebotom • Life cycle : Animals – Phlebotom - Humans • Anthroponotic VL (AVL): • Reservoir: Humans • Vector: Phlebotom • Life cycle: humans – Phlebotom - Humans CAKIR: LEISHMANIASIS 2014-2015 34
ZVL – AVL: Epidemiologic characteristics • In Past: Genrally ZVL Seldomly AVL • Nowadays: ZVL-AVL Common • Günümüzde etken frkları • L infantum: Still ZVL • L donovani: AVL biçiminde bulaşır CAKIR: LEISHMANIASIS 2014-2015 35
Visceral leisahmaniasis: (VL) • Patinets from endemic area • Insidious onset and turn to chronic phase • Patients from non-endemic area and history of endemic area visits • Acute onset • In some African cases dermal granulomas can be detected • Clinical picturee: • Persistant intermittent fever, • Weigh loss, • Loss of apetite, • Anemia, • Abdominal discomfort • Hepato-splenomegaly CAKIR: LEISHMANIASIS 2014-2015
Causes of anemia in VL • Persistan inflamatory stage • Hipersplenism • Bleedings CAKIR: LEISHMANIASIS 2014-2015 37
VL • Thrombositopenia: Petechia hemorrhage or mucosal bleeding • Leucopenia: Secondary infections • Other findings: Cough, chronic diarrhoea, skin hyperpigmentation, lymphadenopathychronic renal involvement • Mild clinical forms can heal spontaneously. • Untreated cases: secondary complications fatal outcome • Fulminant and fatal cases: • In HIV Co-infections • Asymptomatic infections: • Some patints may present live parasite despite adequate treatment • Asymptomatic carrier state + Immune defficiency
Kala azar pentade • Fever • Weigh loss • Organomegalies: Soft and palpable • Pansitopenia Severe thrombocytopenia epistaxis, petechias • Hypergamaglobulinemia CAKIR: LEISHMANIASIS 2014-2015
Geographic varations of VL’s clinical pictures Clinical findings can be changed due to geographic area • Lymphadenopathy: • Seldom in India • Frequent in Sudan Sudan • Dermal hyperpigmentation • Frequent in India • Only during prolonged infections in other endemic regions • Conclusion: Regional symptomatic varaiations should be determined by authorities CAKIR: LEISHMANIASIS 2014-2015 40
Outcome of VL • Splenomagaly may increase in delayed phase • Abdominal symptoms: • Abdominal swelling • Gastric pain • Hepatomegaly • Bacterial co-infections: Pneumonia, diarrhoea, activation of tuberculosis • Untreated patients: • Primary outcomes: • Secondary infections: Bacterial co-infections Few weeks – few months CAKIR: LEISHMANIASIS 2014-2015 41
VL’de epidemic polymorphism No relations between contamination and (Apparent, clinical) infection..... ( Rate is not 1:1) • Asymptomatic infection: Apparent infection rates • Sudan1:2,62 11:1’e • Kenya: 4:1 • Etiopia 5,6:1 • Iran 13:1, • Brasil 8:1 18:1 • Spain 50:1 • Q: Why are immunisation programs unsuccesful for some persons ? • Q: Why are there a difference between contamination and infection? Neden her etkeni alan hastalanamaz? • A: Host-spesific cellulary immunity has great effect on clinical pictures CAKIR: LEISHMANIASIS 2014-2015 42
Etiology: L. donovani After recovery of VL In some patients Peri-oral area Maculopapullary, Macular or nodullary rashes African patient Can be seen in... 6. moths Spontaneus healing even if not trated Successful treatment cannot prevent PKLD Post-kala azar dermal leishmaniasis (PKDL): CAKIR: LEISHMANIASIS 2014-2015
(PKDL) • One of complication of VL • Common in Sudan • Less frequent in other Eastern African countries and Indian subcontinent • Immuncompromised patients in L infantum endemic area • Very contagious vivid parasites present in nodulary lesions CAKIR: LEISHMANIASIS 2014-2015 44
Genetic characteristics of tendency to VL • Severe T-cell irresponsiveless to L donovani antigens • İnterleucin 10 production , CD25-Foxp3 that responsible to secret them • Concomitant diseases like Malnutrition and HIV that altered immun reactions • Others • Young ages • Diminished interferon-X production, • TNF –y gene-40 Promoter polymorfism • Controlling factors on macrophage activation: • Solute taşıcarrier gene family11 A1 (SLC11A1; previously NRAMP1) • Gene poliymorphism controls L4 productions CAKIR: LEISHMANIASIS 2014-2015 45
Preventing strategies VL • Two control srategies : • Controlling of reservoir • Vector controll kontrolü • Immunisation programs still ongoing CAKIR: LEISHMANIASIS 2014-2015 46
Control of reservoirs • ZVL: L. İnfantum main reservoirs: Canines • Gradually ZVL decreases • Serologic sreening of canines ???? • Treatment or killing the seropositive-animals ???? • C0mments: • Animal treatment will not stop re-infections • Widely use of anti -ZVL drugs will cause resistant strains ilaçlarının yaygın kullanımı dirence yol açar • Protection of domerstic animals :Deltamethrin impregnated dog-collars • Prevention of animals from phlebotoms (54%) • Can be adopted to school collar stud: Prevents children: (43%)
Vector control • Insecticides : Effect,ve on Phlebotomes and pther mosquitos • Ör: DDT • Disadvantage: Repeated growth of mosquitos • resistance to insecticides İnsektis • Alternatives : DDT embedded nets CAKIR: LEISHMANIASIS 2014-2015 48
Early diagnosis and treatment: • Goal of early diagnosis and treatment: • Prevents new cases • Patient’s health • Prevention of AVL cases • Management of aditional problems: • Anemia, • Malnutrition • Treatmen of secondary infections CAKIR: LEISHMANIASIS 2014-2015 49
Diagnosis: Non-leishmanial tests • Pancytopenia (anemia, eucopeniai vehrombocytopenia) • Bu bulgunun özgünlüğü yüksek (%98) • Duyarlılığı düşük (%16) • Formol gel test (FJT) or aldehyde test: • Detects typical polyclonal hipergamaglobulinemias • Easy and chip • Low sensitivity (35%) CAKIR: LEISHMANIASIS 2014-2015 50