Download
1 / 1
10 likes | 104 Views
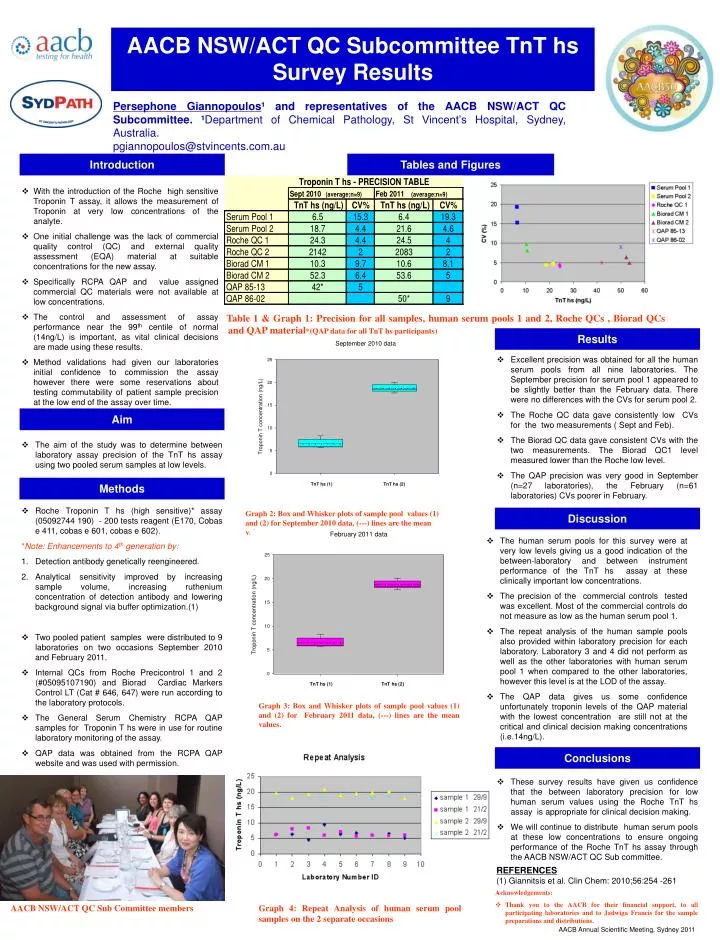
AACB NSW/ACT QC Subcommittee TnT hs Survey Results. Persephone Giannopoulos ¹ and representatives of the AACB NSW/ACT QC Subcommittee. ¹ Department of Chemical Pathology, St Vincent’s Hospital, Sydney, Australia. pgiannopoulos@stvincents.com.au. Introduction. Tables and Figures.

E N D
AACB NSW/ACT QC Subcommittee TnT hs Survey Results Persephone Giannopoulos¹ and representatives of the AACB NSW/ACT QC Subcommittee. ¹Department of Chemical Pathology, St Vincent’s Hospital, Sydney, Australia. pgiannopoulos@stvincents.com.au Introduction Tables and Figures • With the introduction of the Roche high sensitive Troponin T assay, it allows the measurement of Troponin at very low concentrations of the analyte. • One initial challenge was the lack of commercial quality control (QC) and external quality assessment (EQA) material at suitable concentrations for the new assay. • Specifically RCPA QAP and value assigned commercial QC materials were not available at low concentrations. • The control and assessment of assay performance near the 99th centile of normal (14ng/L) is important, as vital clinical decisions are made using these results. • Method validations had given our laboratories initial confidence to commission the assay however there were some reservations about testing commutability of patient sample precision at the low end of the assay over time. Table 1 & Graph 1: Precision for all samples, human serum pools 1 and 2, Roche QCs , Biorad QCs and QAP material*(QAP data for all TnT hs participants) Results • Excellent precision was obtained for all the human serum pools from all nine laboratories. The September precision for serum pool 1 appeared to be slightly better than the February data. There were no differences with the CVs for serum pool 2. • The Roche QC data gave consistently low CVs for the two measurements ( Sept and Feb). • The Biorad QC data gave consistent CVs with the two measurements. The Biorad QC1 level measured lower than the Roche low level. • The QAP precision was very good in September (n=27 laboratories), the February (n=61 laboratories) CVs poorer in February. Aim • The aim of the study was to determine between laboratory assay precision of the TnT hs assay using two pooled serum samples at low levels. Methods • Roche Troponin T hs (high sensitive)* assay (05092744 190) - 200 tests reagent (E170, Cobas e 411, cobas e 601, cobas e 602). *Note: Enhancements to 4th generation by: • Detection antibody genetically reengineered. • Analytical sensitivity improved by increasing sample volume, increasing ruthenium concentration of detection antibody and lowering background signal via buffer optimization.(1) • Two pooled patient samples were distributed to 9 laboratories on two occasions September 2010 and February 2011. • Internal QCs from Roche Precicontrol 1 and 2 (#05095107190) and Biorad Cardiac Markers Control LT (Cat # 646, 647) were run according to the laboratory protocols. • The General Serum Chemistry RCPA QAP samples for Troponin T hs were in use for routine laboratory monitoring of the assay. • QAP data was obtained from the RCPA QAP website and was used with permission. Graph 2: Box and Whisker plots of sample pool values (1) and (2) for September 2010 data, (---) lines are the mean values. Discussion • The human serum pools for this survey were at very low levels giving us a good indication of the between-laboratory and between instrument performance of the TnT hs assay at these clinically important low concentrations. • The precision of the commercial controls tested was excellent. Most of the commercial controls do not measure as low as the human serum pool 1. • The repeat analysis of the human sample pools also provided within laboratory precision for each laboratory. Laboratory 3 and 4 did not perform as well as the other laboratories with human serum pool 1 when compared to the other laboratories, however this level is at the LOD of the assay. • The QAP data gives us some confidence unfortunately troponin levels of the QAP material with the lowest concentration are still not at the critical and clinical decision making concentrations (i.e.14ng/L). Graph 3: Box and Whisker plots of sample pool values (1) and (2) for February 2011 data, (---) lines are the mean values. Conclusions • These survey results have given us confidence that the between laboratory precision for low human serum values using the Roche TnT hs assay is appropriate for clinical decision making. • We will continue to distribute human serum pools at these low concentrations to ensure ongoing performance of the Roche TnT hs assay through the AACB NSW/ACT QC Sub committee. REFERENCES (1) Giannitsis et al. Clin Chem: 2010;56:254 -261 . Acknowledgements: • Thank you to the AACB for their financial support, to all participating laboratories and to Jadwiga Francis for the sample preparations and distributions. AACB NSW/ACT QC Sub Committee members Graph 4: Repeat Analysis of human serum pool samples on the 2 separate occasions AACB Annual Scientific Meeting, Sydney 2011