Download
1 / 13
170 likes | 536 Views
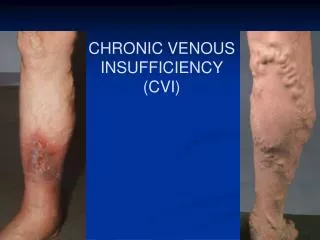
Venous thromboembolism – Treatment and secondary prevention. DVT. PE. Deep vein insufficiency. Post-thrombotic syndrome. Pulmonary hypertension. Death. Ulcus cruris. Chronic PE. Deep vein thrombosis. Common femoral vein. Thrombus. Proximal. Knee. Distal.

E N D
Venous thromboembolism – Treatment and secondary prevention DVT PE Deep vein insufficiency Post-thrombotic syndrome Pulmonary hypertension Death Ulcus cruris Chronic PE
Deep vein thrombosis Common femoral vein Thrombus Proximal Knee Distal
Treatment and secondary prevention of VTE VTE event Acute Continue Heparin or LMWH together with a VKA (e.g. warfarin) until an INR of 2.0-3.0 is achieved VKA (e.g. warfarin)INR 2.0-3.0
VTE - treatment options Acute Long-term • Anticoagulation - UFH/LMWH • Thrombolysis • Thrombectomy • Inferior vena cava filters (IVCF) • Anticoagulation- VKAs (e.g. warfarin)- LMWH • Stockings
7th ACCP recommendations- Initial treatment for acute DVT or PE • Confirmed DVT or non-massive PE • Initial treatment with sc LMWH or iv UFH (or sc if DVT) [Grade 1A] for at least 5 days [Grade 1C] • Start VKA with LMWH or UFH on day 1 [Grade 1A] • Stop LMWH or UFH when INR stable >2.0 [Grade 1A] • High clinical suspicion of VTE • Anticoagulation until outcome of diagnostic tests [Grade 1C+] Büller H et al. Chest 2004;126:401S–428S
Treatment and secondary prevention of VTE VTE event Decision point How long? Acute Continue Heparin or LMWH together with a VKA (e.g. warfarin) untill an INR of 2.0-3.0 is achieved VKA (e.g. warfarin)INR 2.0-3.0 3-6-12 months or lifelong Risk of VTE (5-7%/year) vs. Risk of bleeding (3-4%/year)
7th ACCP recommendations- Long-term treatment for DVT or PE • First episode with a transient risk factor • 3 months after distal or proximal DVT [Grade 1A] • At least 3 months after PE [Grade 1A] • First episode of idiopathic DVT/PE • VKA for at least 6–12 months [Grade 1A] but consider indefinite duration [Grade 2A] • Two or more episodes of DVT/PE • Suggest indefinite treatment [Grade 2A] • Target INR 2.5 (range 2.0–3.0) [Grade 1A] Büller H et al. Chest 2004;126:401S–428S
Long-term treatment of DVT • Recurrence rate of VTE in patients with DVT dependent on – Underlying risk factors for DVT – Duration of treatment • Decision regarding duration of treatmentdependent on – Underlying risk factors for DVT – Risk of haemorrhage from oral anticoagulation– Patient preference • Numerous regimens studied to improve benefit of long-term treatment while reducing the dose
Recurrence of VTE after stopping oral anticoagulation 3 months treatment Event rate (%) 15 10 5 0 0 3 6 12 24 Months
Recurrence of VTE after stopping oral anticoagulation 3 months treatment Event rate(%) 6 months treatment 15 10 5 0 0 3 6 12 24 Months
Recurrence of VTE after stopping oral anticoagulation 3 months treatment Event rate(%) 6 months treatment 1 year treatment 15 10 5 0 0 3 6 12 24 Months
Optimal duration of anticoagulation after VTE LongOAC ShortOAC Reference No. ofpatients Followup Recurrent VTE Major bleeding months months months LongOAC ShortOAC LongOAC ShortOAC DURAC I 897 6 1.5 24 9.5% 18.1% 1.1% 0.2% LAFIT 162 27 3 10 1.3% 27.4% 3.8% 0.0% WODIT-DVT 267 12 3 12 3.0% 8.3% 3.0% 0.8% WODIT-PE 326 6-12 3 32.7 4.1% 9.1% 1.8% 0.0% DOTAVK 539 6 3 15 8.7% 8.1% 2.6% 1.9% DURAC II 227 Indefinite 6 43 2.6% 20.7% 8.6% 2.7% OAC, oral anticoagulation
Intensity of anticoagulant therapy Recurrent VTE Cumulative event rate (%) 0.25 Placebo - PREVENT 0.20 0.15 Low INR – PREVENT 0.10 Low INR – ELATE 0.05 Conventional INR - ELATE 0.00 0 1 2 3 4 Years of follow-up Ridker PM et al. N Engl J Med 2003; 348:1425-34 Kearon C et al. N Engl J Med 2003;349:631-9