Download
1 / 10
110 likes | 122 Views
Explore the historical background and current status of Medicare Advantage plans, with a focus on key legislative changes and enrollment data. Learn about plan types, premiums, out-of-pocket costs, and beneficiary distribution.

E N D
Medicare Advantage: Background and Current Status by Marsha Gold, Sc.D. Senior FellowMathematica Policy Research, Inc. May 4, 2008 Presented at Alliance for Health Reform Briefing
Origins of Medicare Advantage • TEFRA of 1982 (effective 1985): Medicare Risk Contracting (HMO) Program • BBA of 1997: Medicare+Choice (additional local coordinated care choices, PFFS, rate floors and other changes); subsequent refinements (BIPA and others) • MMA of 2003: immediate payment changes (increases) 2004-2005, SNPs • MMA of 2003 (effective 2006): Part D, regional PPOs, MSAs, payment benchmarks
Medicare Private Plan Enrollment by Contract Type, 1999–2009 Source: CMS Monthly Summary Report, December various years; March for 2009. Note: “Other” include 1876 cost plans, 1833 cost plans (HCPPS), PACE and demonstrations.
Percentage of Beneficiaries with MA Choice in Urban and Rural Areas, 1999-2009 Urban Counties Rural Counties Source: MPR analysis of publicly available CMS data.
Percentage of Beneficiaries by Number of Firms Competing for MA Business, 2009 Source: MPR analysis of CMS data from the Contract-County file for March 2009. Excludes sponsors offering group-only products. CCP = HMO and PPO aIncludes 12 percent with no choice, 12 percent with 1 sponsor choice, 11 percent with 2 choices, and 24 percent with 3-4 choices.
Distribution of Total MA Enrollment by Firm or Affiliate, 2009 a Source: MPR analysis of CMS’s Contract-County file for March 2009. aWellPoint has a 4 percent market share including BC-BS affiliates. (BC-BS has 14.3 percent without WellPoint.)
MA-PD Premiums by Plan Type (Weighted by Enrollment), 2009 Source: MPR analysis of CMS’s Medicare Options Compare, CMS’s March 2009 enrollment data. Note: Statistics exclude group and SNP plans.
Estimated Annual Out-of-Pocket Costs for Hospital and Physicians Services Differ by Plan Type and Enrollee Health Status, 2009 Source: MPR analysis of CMS’s Medicare Options Compare data. Uses assumptions of hospital and physician use based on HealthMetrix Note: Statistics are enrollment-weighted (March 2009) and exclude group and SNP plans. aAssumes a mix of 72 percent healthy, 19 percent with episodic needs, and 9 percent with chronic needs, which is equal to the distribution of community-residing beneficiaries in good, fair, and poor health. bAssumes enrollees’ use of in-network benefits. Includes provider-sponsored plans.
Distribution of Beneficiaries by Number of Individual MA Plans Available, 2009 Source: MPR analysis of CMS data. Note: Excludes SNP and group plans.
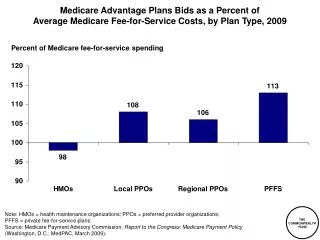
Where We Are Now • MA enrollment now almost a quarter of beneficiaries and adds to Medicare costs • PFFS disporportionately accounts for growth (and availability in rural areas) • Many firms compete but most enrollment concentrated in a few • Premiums are attractive but financial risk remains • Beneficiaries asked to distinguish numerous and diverse plans.