Download
1 / 53
540 likes | 562 Views
Delve into the intricacies of thyroid function and how drugs can impact the interpretation of diagnostic tests. Learn about the thyroid gland, follicles, key elements, feedback mechanisms, and clinical features of thyroid disease. Discover the regulation of thyroid hormone synthesis and metabolism in the body.

E N D
Dr Asad Vaisi-Raygani Professor in Clinical Biochemistry Drugs interferes with Interpretation of Thyroid Diagnostic Tests
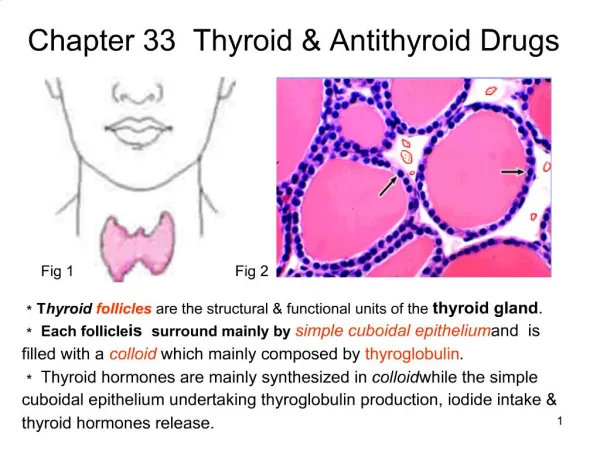
Where to look for Thyroid ? The thyroid is a butterfly-shaped gland located in the front of the neck just above the trachea that weighs approximately 15 to 20 grams in the adult human
Follicles: the Functional Units of the Thyroid Gland Follicles Are the Sites Where Key Thyroid Elements Function: • Thyroglobulin (Tg) • Tyrosine • Iodine • Thyroxine (T4) • Triiodotyrosine (T3)
Thyroperoxidase TPO Tiouracil methylmazol I- , ClO2- CN- , SCN-
At least 85% of normal T3 production and essentially all of rT3 production can be accounted for by peripheral deiodination of T4 rather than by direct secretion by the thyroid gland.T3 is four to five times more potent in biological systems than T4 (prohormone).
Hypothalamic-Pituitary-Thyroid AxisNegative Feedback Mechanism negative feedback positive feedback
The β2 receptor(β2AR) (β2adrenoreceptor) Activation of β adrenergic receptors leads to relaxation of smooth muscle in the lung, and dilation and opening of the airways. β adrenergic receptors) is unique to the pituitary gland and is central in the negative-feedback regulation of TSH by thyroid hormone. The α2 receptor (example كلونيدين ) is inhibitory and acts as a negative regulator of thyroid hormone action. Mutations in the β receptors, which diminish the ability of T3 to bind to the nucleus, have been described in the syndrome of thyroid hormone resistance. Individuals with this syndrome have growth and mental retardation of varying degrees, as well as hypothyroidism (Refetoff, 1991)
Synthesis of thyroid hormones is regulated by pituitary TSH which stimulates the "iodide pump," Tg synthesis, and colloidal uptake by follicular cells. TSH also regulates the rate of proteolysis of Tg for the liberation of T3 and T4. TSH induces an increase in the size and number of the thyroid follicular cells. Prolonged TSH stimulation leads to increased vascularity and eventual hypertrophic enlargement of the thyroid gland (goiter).
Metabolism In the liver, T4 and T3 are conjugated to form sulfates and glucuronides. These conjugates enter the bile and pass into the intestine. Thyroid hormone conjugates are hydrolyzed, and some are reabsorbed (enterohepatic circulation) or excreted in the stools.
T4 and T3 are carried in the circulation bound to carrier proteins. These carrier proteins (thyroxin-binding globulin TBG], thyroxin-binding prealbumin TBPA], and albumin) bind 99.97% of T4 and 99.7% of T3.
Heroin and methadone Phencyclidine, heparin, barbital
Clinical features of thyroid disease • The three common presentations of thyroid disease are: • 1. Hyperthyroidism (229) • 2. Hypothyroidism (230) • 3. Goitre (231) which may be non-toxic or associated with hyperthyroidism or hypothyroidism.
1. Hyperthyroidism(229)2. Hypothyroidism (230) 3. Goitre (231) which may be non-toxic or associated with hyperthyroidism or hypothyroidism.
Thyroid Dysfunction Laboratory testing of thyroid hormones is used to diagnose and document the presence ofHypothyroidism and hyperthyroidism
Hypothyroidism Hypothyroidism is defined as a deficiency in thyroid hormone secretion and action. It is a common disorder that occurs in mild or severe forms in 2% to 15% of the population. Women are afflicted more often than men, and both sexes are affected more frequently with increasing age.
Myxedema is a severe form of hypothyroidism in which there is accumulation of mucopolysaccharides in the skin and other tissues, leading to a thickening of facial features and a doughy indurations of the skin. Cretinism is the term used to describe severe hypothyroidism that develops in the newborn period.
Hypothyroidism caused increased TSH • Inhibited dopamine • Dopamine stimulated GH • Dopamine inhibited secretion of prolactin • hormones such as testosterone, estrogens, and thyroxine, all stimulate GH secretion
Amidodarone is derivate of benzophenon used for treatment of anti arrhythmic Of ventricular
Primary hypothyroidism is frequently caused by diseases or treatments that directly destroy thyroid tissue or interfere with thyroid hormone biosynthesis. T4 decrease Hypoprotenemia(eg. Nehprotic, cirrhosis) certain drugs, phenytoin, T3, Testestrone, ACTH, corticoidsteroides and Euthyroid sick syndrome decrease TBG Secondary hypothyroidism occurs as a result of pituitary (TSH deficiency) or hypothalamic (TRH deficiency) disease and/or disorders.
Primary Hypothyroidism Primary goitrous hypothyroidism results when the synthesis of T4 and T3 is impaired, either because of some extrinsic factor or because of an intrinsic, inherited defect in thyroid hormone biosynthesis. As a result, the positive feedback loop causes compensatory thyroid enlargement (goiter) through the hypersecretion of TRH and TSH.
Primary nongoitrous hypothyroidism is characterized by loss or atrophy of thyroid tissue, resulting in decreased production of thyroid hormones despite maximum stimulation by TSH (surgical removal or radioablation). Autoimmune Hashimoto's thyroiditis (goitrous) is the most frequent cause of primary hypothyroidism in developed countries where iodine intake is sufficient. Worldwide, iodine deficiency is the most common cause of goitrous hypothyroidism.
Primary hypothyroidism is frequently associated with circulating antithyroid antibodies and may coexist with other diseases in which autoantibodies are found.
Reduced concentrations and availability of T4 and T3 lead to hypersecretion of pituitary TSH and marked elevations in serum TSH concentrations. The elevated concentration of TSH is an important laboratory finding particularly in the early detection of thyroid failure.(ref range 0/4-6 IU/L >6 possible hypo and <0/1 possible hyper,Borderline; 0/1- 0/39 Increase by amphetamine, drugs contain iodine, dopamine antagonist(metochlopramide, choropromazine(largagtil, haptopridol) pituitary resistance to thyroid hormon In mild or subclinical hypothyroidism thyroid hormone concentrations can remain within the normal reference interval but the TSH concentration is elevated.
Drugs such as high dose glucocorticoids , dopamine, • dopamine agonist (bromocriptine) levodopa, apomorphine,
Primary hypothyroidism is easily treated by the daily administration of oral thyroxine. During initial treatment, serum FT4 concentrations adjust quickly, but TSH concentrations remain high. Because the pituitary is slow to register acute changes in thyroid hormone status ("pituitary lag"), 4 to 8 weeks may be needed for serum TSH values to reach a new steady state after dose adjustments. Periodic monitoring of serum TSH (1 to 3 times a year) is recommended.
Secondary Hypothyroidism Secondary hypothyroidism (central thyroid disease) occurs as a result of pituitary or hypothalamic diseases that produce a deficiency in either TSH, TRH, or both. Most patients with secondary hypothyroidism also have other pituitary hormone deficiencies as well (panhypopituitarism). With secondary hypothyroidism, the serum concentration of thyroid hormone is low, but TSH concentrations are either low or within the normal reference interval.
Partial or complete failure of pituitary hormone production (1)
Hyperthyroidism • Hyperthyroidism is the clinical condition that results from increased • circulating levels of free thyroid hormones. The causes of hyperthyroidism,
Pregnancy, methadone heroin ,estrogens Amphetamine radiopaque, ,
Biochemical picture of primary hyperthyroidism shows increases in T4 and T3' with a TSH suppressed to undetectable concentrations, except in those rare cases in which hyperthyroidism is mediated by TSH itself. Patients with hyperthyroidism typically have serum TSH concentrations less than 0.05 mIU/L. A serum TSH within the euthyroid reference interval almost always eliminates the diagnosis of hyperthyroidism.
Finding a low TSH concentration and an elevated FT4, concentration is usually sufficient to establish the diagnosis of hyperthyroidism. If the TSH concentration is low but the FT4 is within the normal reference interval, a T3 measurement should be performed, because serum T3 concentration is often elevated to a greater degree than T4. T-3 toxicosis causes is 5% of hyperthyroidism A suppressed serum TSH concentration, associated with normal concentrations of serum T3 and FT4 may signify "subclinical hyperthyroidism," when the individual is asymptomatic.
Occasionally, increases in serum concentrations of T4 and T3 will occur as a result of the ingestion of large quantities of exogenous thyroid hormones or to the release of thyroid hormones as a result of damage to the thyroid parenchyma associated with subacute thyroiditis or chronic lymphocytic thyroiditis.
Treatment is typically designed to decrease thyroid hormone production or inhibit peripheral conversion of T4 to T3 (propylthiouracil and methimazole). When treatment is initiated, measurements of serum FT4 are recommended every few weeks until symptoms abate and serum values normalize. Serum TSH is not a good monitor of thyroid status in the immediate period following the start of antithyroid therapy and remain undetectable for months after the patient becomes clinically euthyroid.
Effect of Drugs A number of medications have been shown to alter thyroid function and thyroid function tests. Glucocorticoids and dopamine reduce TSH but amiodarone increased TSH concentrations. The most commonly encountered variations in thyroid hormone measurements induced by medications are reduced peripheral conversion of T4 to T3 or altered binding of T4 and T3 to carrier proteins.
Traditionally, thyroid testing has been performed with T4 or free thyroxin estimate(FT4E) however these tests are not ideal indicators of thyroid status: 1. Variations in serum binding protein concentrations 2. T3 is the primary active of thyroid hormone The relationships between T4 and T3 are not always predictable. In patients with hyperthyroidism, T3 is usually elevated to a greater extent than T4 because it is derived from two sources; increased thyroidal secretion of T3 and increased peripheral conversion of T4 to T3.
The serum concentration of TSH reflects the integrated action of thyroid hormones at the concentration of one of its target tissues-the pituitary cells that secrete TSH. Pituitary TSH secretion is very sensitive to circulating thyroid hormone concentrations; in fact, a twofold change in FT4 cause a 100-fold change in the serum TSH concentration.
The major clinical roles for total T3 measurements are in the diagnosis and monitoring of hyperthyroid patients with suppressed TSH and normal FT4 concentrations (T3-thyrotoxicosis); T3 measurements have only a limited role in euthyroid and hypothyroid patients.
Specimen Collection and Storage Serum or plasma is used for the measurement of TSH and the thyroid hormones, with serum free of hemolysis and lipemia preferred. Specimens are stable for 5 days at 2 °C to 8 °C and for at least 1 month when stored frozen.