Download
1 / 31
310 likes | 513 Views
REPRODUCTIVE AGE GROUP. AUB. Normal Menses . The mean duration of menses is 4.7 days; 89% of cycles last 7 days or longer. The average blood loss per cycle is 35 ml . the blood content of menses varies over the days of bleeding, but on average is close to 50% .

E N D
Normal Menses • The mean duration of menses is 4.7 days; 89% of cycles last 7 days or longer. • The average blood loss per cycle is 35 ml . • the blood content of menses varies over the days of bleeding, but on average is close to 50% . • Recurrent bleeding in excess of 80 ml /cycle results in anemia
Prevalence • %5 of women between the age 30 and 49 years consult a physician for menorrhagia . • 21 to %67 develops iron deficiency anemia .
Differential diagnosis • dysfunctional uterine bleeding (estrogen breakthrough. Low levels of estrogen stimulation whereas higher sustained levels result in episodes of amenorrhea followed by acute, heavy bleeding. • Pregnancy-related Bleeding. In the United States, more than 50% of pregnancies are unintended. • EP.
Differential diagnosis • Exogenous Hormones . • Ocpill. contraceptive patch, vaginal ring, and intramuscular regimens, • Use of progestin-only methods—including DMPA, progestin-only pills, the contraceptive implant, and the levonorgestrel IUS. is associated with relatively high rates of initial irregular and unpredictable bleeding .
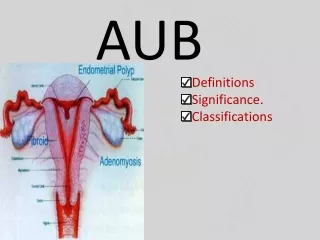
Causes of abnormal genital tract bleeding • Genital tract disorders : uterus • polyps • endometrial hyperplasia • Adenomyosis • fibroids • adenocarcinoma • sarcoma • endometritis • anovulatory bleeding
Systemic disease • Crohn's disease • Behcet's syndrome • PemphigoidPemphigus • Erosive lichen planus • Lymphoma • Coagulation disorders: • von Willebrand's disease
Systemic disease • Hormone secreting adrenal and ovarian tumors • Renal disease • Emotional or physical stress • Smoking • Excessive exercise
Systemic disease • Diseases not affecting the genital tract • Urethritis • Bladder cancer • Urinary tract infection • Inflammatory bowel disease • Hemorrhoids • Vascular tumors and anomalies in the genital tract
Endocrine Causes • hypothyroidism and hyperthyroidism . • With hypothyroidism : Menorrhagia, are common. • Hyperthyroidism can result in oligomenorrhea or amenorrhea. and it also can lead to elevated levels of plasma estrogen. • Hypothalamic dysfunction, hyperprolactinemia, premature ovarian failure, and primary pituitary disease, irregular bleeding also may result in their presence.
Endocrine Causes. • Diabetes mellitus can be associated with Anovulation, obesity, insulin resistance, and androgen excess . • Polycystic ovary syndrome is present in 5% to 8% of adult women and undiagnosed in many women . • Because androgen disorders are associated with significant cardiovascular disease, the condition should be diagnosed promptly and treated.
Anatomic Causes • Uterine leiomyomas. cumulative prevalence of greater than 80% in black women and nearly 70% in white women. are estimated to be clinically significant in at least 25%of women of reproductive age. • Endometrial polyps. :are a cause of intermenstrual bleeding, irregular bleeding, and Menorrhagia, although as with leiomyomas, most endometrial polyps are asymptomatic. • Endometrial polyps can regress spontaneously. • the chance of malignancy is less than 5% and likely approximates 0.5%
Abnormal bleeding • intermenstrual or postcoital, • Cervical lesions. • endocervical polyps. • infectious cervical lesions, such as condylomata, herpes simplex virus, ulcerations, chlamydialcervicitis, or cervicitis caused by other organisms.
Coagulopathies and Hematologic Causes • A complete blood count will be helpful in detecting anemia, significant problems such as leukemia or disorders associated with thrombocytopenia. • Alcoholism . • von Willebrand's disease. • Oral contraceptive ,
Infectious Causes • Cervicitis: • chlamydialcervicitis, can experience irregular bleeding and postcoital spotting • Endometritis can cause excessive menstrual flow. • woman who seeks treatment for menorrhagia and increased menstrual pain and has a history of light-to-moderate previous menstrual flow may have an upper genital tract infection or PID (endometritis, salpingitis, oophoritis). • chronic endometritis will be diagnosed when an endometrial biopsy is obtained for evaluation of abnormal bleeding in a patient without specific risk factors for PID.
Neoplasia • invasive cervical cancer. • cervical lesion should be evaluated by biopsy, testing may be falsely negative with invasive lesions as a result of tumor necrosis. • Unopposed estrogen of the endometrium: cystic hyperplasia to adenomatous hyperplasia, hyperplasia with cytologicatypia, and invasive carcinoma. • Vaginal neoplasia is uncommon
Diagnosis • exclusion of pregnancy.CBC diff. PT,PTT, prothrombin time and partial prothrombin time ,von Willebrand´s disease . • possible malignancy. • imaging studies. measurements of endometrial thickness are significantly Less useful in premenopausal than postmenopausal women. • Sonohysterography is especially helpful in visualizing intrauterine problems such as polyps or submucous leiomyoma. • CT scanning and MRI, are not as helpful in the initial evaluation of causes of abnormal bleeding and should be reserved for specific indications.
Endometrial Sampling • Endometrial sampling should be performed to evaluate abnormal bleeding in women who are at risk for endometrial polyps, hyperplasia, or carcinoma. D & C, Hysteroscopy, endometrial sampling,
Management • medical therapy . • surgical management . • endometrial ablation • hysterectomy
Nonsurgical Management • NSAIDs .Mefenamic acid 500 mg three times per day • Naproxen 500 mg at onset and three to five hours later, then 250 to 500 mg twice a day • Ibuprofen 600 mg once per day. • Antifibrinolytics;tranexamic acid .amincaproic acid. • Levonorgestrel-containing intrauterine devices . • Oral contraceptives, Ocs E²>35mcg than 20mcg. • For patients in whom estrogen use is contraindicated, progestins, both oral and parenteral, can be used to control excessive bleeding .
medroxyprogesterone acetate, administered from days 5 to 26 of the cycle . • Depot formulations of medroxyprogesterone acetate • Oral, parenteral, or intrauterine delivery of progestins may be used in selected women with atypical endometrial hyperplasia who wish to maintain their fertility, continued monitoring every 3 month is indicated . • Danazol . • Gonadotropin-releasing hormone analogues . • levonorgestrel-containing IUS .
Surgical Therapy • D&C . • Endometrial ablation or resection . • Hysterectomy . • Hysteroscopy . • Laparoscopy . • Uterine artery Embolization . • Magnetic resonance guided focused ultrasonography ablation .