Download
1 / 36
370 likes | 813 Views
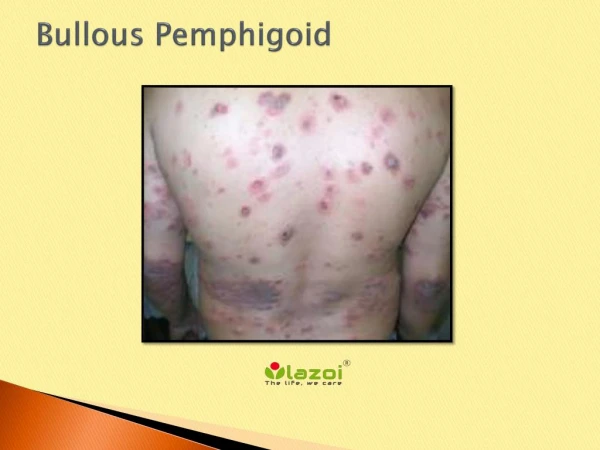
Incidence and mortality of bullous pemphigoid and pemphigus vulgaris in the UK. Sin éad Langan Joe West. Bullous pemphigoid. Incidence rates between 0.2 and 3 per 100,000 person-years Estimated incidence of 1.4 per 100,000 person-years in Scotland Reported 1-year mortality rates

E N D
Incidence and mortality of bullous pemphigoid and pemphigus vulgaris in the UK Sinéad Langan Joe West
Bullous pemphigoid Incidence rates between 0.2 and 3 per 100,000 person-years Estimated incidence of 1.4 per 100,000 person-years in Scotland Reported 1-year mortality rates between 6% (USA) and 41% (France)
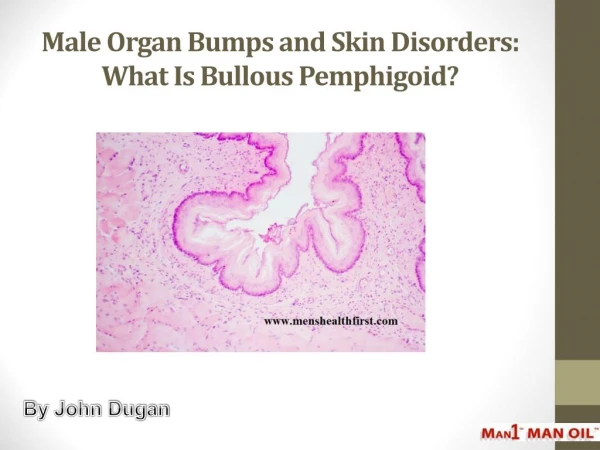
Pemphigus vulgaris Few studies, incidence between 0.08 and 1.6 per 100,000 person-years No data from the UK 1 year mortality rates between 4.8 and 54%; no clear estimate of overall disease- specific mortality rates
Objectives To determine incidence and mortality of bullous pemphigoid and pemphigus vulgaris in the United Kingdom (UK)
Data source Computerised medical records from the Health Improvement Network (THIN), a large population-based UK general practice database were analysed
Confounders • Age group in 10 year bands • Gender • Region • Townsend scores
Study populations • All patients >20 years with bullous pemphigoid and pemphigus vulgaris diagnosed 1996-2006 • First 3 months following registration excluded • 4 matched controls selected per case
Incidence • Incidence rates by age category, gender and calendar period • Incidence rate ratios (IRR) adjusting for changes in age, gender structure and calendar period over time
Mortality • Deaths in cases and controls • Kaplan-Meier techniques used to calculate 1 year mortality and 5 year survival rates • Cox regression to compare mortality experience of cases and controls
ONS data Incidence and mortality rates from this study applied to ONS population data to calculate expected numbers of new cases and number of deaths
Bullous pemphigoid • 868 people with bullous pemphigoid and 3453 matched controls • Median (IQR) age at first presentation for bullous pemphigoid 80 (15) years • 534 (61%) were female
Pemphigus vulgaris • 139 people with pemphigus vulgaris and 551 matched controls • Median (IQR) age at first presentation for pemphigus vulgaris 71 (30) years • 91 (66%) were female
Bullous pemphigoid incidence • Crude incidence= 4.3 (95% CI 4.0-4.6) per 100,000 py • 17% increase per year (IRR 1.2, 95% CI 1.1-1.2), adjusted for gender and age • No association with region or Townsend scores
Bullous pemphigoid mortality 1-year mortality rate=19% (95% CI 16-22) Absolute excess mortality for cases=70 deaths per 1000py Hazard ratios: Crude 2.1 (95% CI 1.8-2.4) Adjusted 2.3 (95% CI 2.0-2.7)
Pemphigus vulgarisincidence • Crude incidence= 0.7 (95% CI 0.6-0.8) per 100,000 py • 11% increase per year (IRR 1.1, 95% CI 1.0-1.2), adjusted for gender and age • No association with region or Townsend scores
Pemphigus vulgarismortality 1-year mortality rate=12% (95% CI 8-19) Absolute excess mortality for cases=62 deaths per 1000py Hazard ratios: Crude 2.8 (95% CI 1.9-4.3) Adjusted 3.4 (95% CI 2.2-5.2)
How many new cases per year? Bullous pemphigoid Applied to ONS data, 2370 new cases per year Pemphigus vulgaris Applied to ONS data, 467 new Cases per year
How many deaths between 2001 and 2005? Bullous pemphigoid Estimated 1977 deaths over 5 years (vs. 190, ONS) Pemphigus vulgaris Estimated 221 deaths over 5 years (vs. 36, ONS)
Key findings • Increased incidence both diseases between 1996 and 2006 • No reduction in mortality rates • Therefore unlikely to be due to ascertainment
Strengths • Large population-based study • Less susceptible to selection bias • Power • Diagnoses usually made with skin biopsy in secondary care • Previous studies confirm validity of diagnoses in THIN • Limited to “up to standard” data
Limitations • Routine data • Cannot comment on disease severity • Possible misclassification of prevalent cases; possible underestimation of mortality rates
Conclusion • Increasing incidence rates over time • No variation by region or socioeconomic status • Mortality rates twice (pemphigoid) and three times (pemphigus) higher than matched controls
Implications • Increasing population age, likely increase in morbidity and mortality from these diseases • Other measures of disease occurrence underestimate associated mortality
Acknowledgements Dr Chris Smith, Professor Liam Smeeth, Dr Kate Fleming and Professor Richard Hubbard Professor Hywel Williams for guidance and support


![[Clinical Case Study II] The treatment for Bullous Pemphigoid at Nimba](https://cdn4.slideserve.com/7791305/slide1-dt.jpg)