Download
1 / 46
470 likes | 1.16k Views
Common Issues in Gynecology: HPV Testing, Bioidentical Hormones, Common Cervical Lesions. Carol A. Stamm MD Director Women’s Services High Street Primary Care Clinical Assistant Professor Medicine UCHSC . HPV Testing: Which of my patients need HPV Testing with their pap?.

E N D
Common Issues in Gynecology: HPV Testing, Bioidentical Hormones, Common Cervical Lesions Carol A. Stamm MD Director Women’s Services High Street Primary Care Clinical Assistant Professor Medicine UCHSC
HPV Testing: Which of my patients need HPV Testing with their pap? • ASCCP Guidelines are evidence-based largely, but rely on expert opinion (29 Professional Societies) for clinical situations in which there is limited high quality evidence. They are guidelines, to be used with physician discretion. No set of guidelines are perfect. • Release of the 2006 ASCCP Consensus Guidelines was delayed 13 months because of continued discussion.
HPV Testing: Which of my patients need HPV Testing with their pap? • After the 2001 ASCCP Guidelines were released, the ASCCP unusually released 2004 Interim Guidelines to suggest how to cope with combined pap and HPV testing. • HPV testing is now more available and the cost is improved. • Recommendations for how to manage combination pap and HPV tests have not been evaluated by a large multidisciplinary group.
HPV Testing: Which of my patients need HPV testing with their pap? • Key follow-up from the NCI-sponsored ASCUS/LSIL Triage Study (ALTS) informs the new guidelines. • Patients with ASCUS pap smear results ( 4-5%)can be effectively triaged for colposcopy by ordering reflex HPV testing for HIGH RISK HPV ONLY. (40-50% +) • This option is not available for conventional pap smears, so that patient must have a follow-up pap at 6 and 12 months. If both tests are negative, continue regular screening. For any higher abnormality, or continued ASCUS, she should be sent to colposcopy. Immediate colposcopy is also an option.
HPV Testing: Which of my patients needs HPV testing with pap? • A patient with an ASCUS pap negative for high risk HPV at any age has a pap good for one year only. Possible explanations: recent coitus, douching, tampon use, infection, recent menses, or trauma or ?… • A patient with an ASCUS pap, positive for HRHPV greater than 20, should be treated as if she has LGSIL, i.e. she should be referred for colposcopy.
HPV Testing: Which of my patients need HPV testing with pap? • ASCUS Cannot Exclude HGSIL, LGSIL, HGSIL should be referred for colposcopy without HPV testing if patient is over 20 years of age. • AGUS patients do not need HPV testing: they need immediate referral to GYN for colposcopy, and possible endometrial biopsy. HPV testing may be obtained at colposcopy. • REPEAT PAP UNACCEPTABLE FOR AGUS.
HPV Testing: Which of my patients need HPV testing with pap? • Adolescents, defined here as less than 20 years of age, are a special case:82% are likely HPV positive /2yrs * • These adolescent guidelines are less evidence-based and are a reaction to the complications (PTL) seen in patients w/ leep prior to pregnancy. • Few invasive cervical cancers are diagnosed in adolescents. • Regression approx 90% 36 months. • Colpo for HSIL still recommended. • Q6 month paps for adolescent with other lesions. • NO NEED TO ORDER HRHPV ON ADOLESCENTS (<20) • *Brown et al JID, 2005
HPV Testing • Revised ACOG Guidelines indicate pap smear screening should begin 3 years after onset of sexual activity and by 21 if not yet sexually active. • The potential impact of the HPV vaccine was not accounted for in the development of these guidelines. Use of the vaccine is less than expected at this time. • Models have predicted different pap smear screening guidelines for women who received complete HPV vaccination in the future.
HPV Testing: Which of my patients needs HPV testing with pap? • Pregnant women w/ LSIL may undergo colpo while pregnant, and have postpartum follow-up if no CIN 2-3 or higher lesion noted, or may defer colposcopy for 6 weeks postpartum. • Adolescents( less than 20) w/ ASCUS or LGSIL may have repeat cytology in a year. This is a significant change, and controversial. You may still send the patient to colposcopy.
HPV testing: Which of my patients needs HPV testing w/ pap? • Patients >=30 years may have pap and HRHPV testing. If both negative, the next pap 3 years. S >99% 10 yr risk CIN 3 1-2% • If the pap is normal and HRHPV is positive, a pap is due in a year. (CIN 2 risk 2-5%-40-60% turn HPV neg w/in 6 months-50-75% by 1 yr) • If the pap is ASCUS and above and HRHPV is positive, colposcopy is needed.
HPV Testing: Who needs HPV w/ Pap? • For women 30 & over who are still HRHPV positive at 1 year, colposcopy is recommended. • HPV 16 pos 20% risk CIN 3 in 10 years • HRHPV testing is Not for Adolescents, twenty-somethings. because of transient colonization & low risk CIN2.
HPV Testing: Which of my patients need HPV testing with pap? • ACOG guidelines have no upper age limit on pap smear screening. • Surprising WHI substudy showed increased risk of pap smear abnormalities in women randomized to HT (.625 mg CEE & 2.5 mg medroxyprogesterone acetate) • 2011 next edition of ASCCP guidelines: Anticipated issues-frequency of pap smear screening in HPV vaccinated individuals…
HPV Testing: Which of my patients needs HPV w/ Pap? • 1. Order it reflexively (i.e. when you get your pap result) if result is ASCUS and if your patient is not less than 20. • 2. Consider it on patients over 30 w/ goal of not doing another pap for 3 years if both tests are negative. • 3. ONLY order HRHPV. The presence of low risk HPV does not cause cancer and only drives up the cost and worries the patient.
HPV Testing • Wright TC et al 2006 Consensus Guidelines for the Management of Women with Abnormal Cervical Cancer Screening Tests. AJOG 2007; 197 (4): 346-355 • Wright TC et al Interim guidelines for the Use of Human Papillomavirus DNA Testing as an Adjunct to Cervical Cytology for Screening. Obstetrics and Gynecology 2004; 103: 367-372 • ASCCP.org
What is the difference in efficacy of bioidenticals/compounded hormones and FDA-approved prescription HT preparations?
“Natural” Estrogen • 17- beta estradiol is the estrogen made by the ovaries primarily before menopause • Estrone is the estrogen most abundant after the menopause • CEE is manufactured from a natural source, horse urine
“Natural” Estrogen Final common pathway of metabolism : 17β -estradiol is metabolized by the liver to estrone
“Natural Estrogen” Neither the NAMS nor the FDA recommend natural over Synthetic estrogen because there is no evidence that ultimate outcomes are different. The recent NIH State-of-the-Science conference on menopausal symptoms concurs. (Inadequate Data and No Safety Data March 2005)
FDA & FTC Warning • Thursday, November 10, 2005 the FDA mailed Warning Letters 16 companies marketing alternative hormone replacement therapies: The treatments are considered to be “unapproved new drugs” • The Federal Trade Commission sent 34 letter to Web Site Operators citing claims that “may be false or unsubstantiated and therefore may violate the law” including progesterone creams, sprays and dietary supplements
FDA & FTC WARNINGS • AllNatural Pain Relief, Bio-health, BuyInnovations.com, CHS International Research, ComCore 21, Greatest Herbs on Earth, HMS Crown, Healthworks 2000, Healthy Days, Heba Laboratores, Herbal Fields Supplements, Nutriteam, One Life USA, Suzanne’s Natural Foods, The Way Up, and Tip Top Vitamins were given 15 days to respond to the FDA www.Kaisernetwork.org Monday, November 14, 2005
Natural Estrogen • January 9, 2008 FDA announced that it warned 7 pharmacies selling “bioidentical” hormones over the Internet that they were breaking the law with false and misleading claims about the benefits • Deborah Autor, FDA Director of Compliance said; “Claims like these mislead consumers and health-care providers with inaccurate information”. • FDA position is that there is no reliable scientific evidence to support the assertions.
OTC Progesterone Creams • Women who rubbed the maximum labeled dose Pro-gest had the same blood levels as those taking Prometrium (J Clin Pharm 2005;45:614) • FDA considering making natural progesterone creams limited to prescription only • No randomized, controlled studies support the safety and efficacy of progesterone cream alone for treatment of menopausal symptoms
Compounding Treatment • “Special for Me” therapy • Allure of “bioidentical” hormones • Adjustment of HT to tenth of a milligram
Compounding Treatment • No outcome data • No evidence for frequent dosage adjustments based on serum testing • No data that saliva testing while taking exogenous hormones is valid • “Normal” premenopausal estradiol is 40-500 pg/ml
FDA Survey 2001www.fda.gov/CDER/pharmcomp/survey.htm • Tested 29 drugs obtained through mail order • 34% of the products failed analytical testing • No data on Colorado compounding pharmacies • NAMS advises not using non-tested formulations when studied options exist
Possible Solutions • Establishing an accreditation process for compounding pharmacies • FDA Advisory Panel for pharmacy compounding • Use caution until steps in places
Compounding Treatment End point should be based on symptom relief, goals of treatment, and risk benefit profile
No Outcome Data: Caution Advised • What is the difference in efficacy of bioidenticals/compounded hormones and FDA-approved prescription HRT preparations? • There are no head-to-head trials. • Most bioidentical and compounded hormones studies do not have a control group. • Known placebo effect of HT studies is 40%.
HT Differences: Compounded vs FDA-Approved • No data other than the progesterone study • Some FDA-Approved options will likely be removed for lack of safety data- estrogen/testosterone formulation specifically. • Data with estradiol suggest serum levels of 80 pg/ml “target range”, but no data for other formulations.
Natural Remedies • Vitamin E 800 IU QD and isoflavones slightly better than placebo • Soy small to no effect • Black cohosh (Cimifuga recemosa) may be helpful – German studies limit to 6 months use although current German practice is more liberal. (Level III Q/A President of European Menopause Society January 2006)
Natural Remedies • Level 1 evidence that long-term soy isoflavone treatment is linked to endometrial hyperplasia • After 5 years of treatment 3.8% of soy treated women had endometrial biopsy demonstrated endometrial hyperplasia( vs RR 8 for unoppposed estrogen) • Isoflavone in soy is similar to estradiol Fertil Steril 2004; 82:145-148, Unfer V, Casini ML, et al
Natural Remedies • Yam cream ineffective but some manufacturers have begun adding progesterone so not all are hormone free. • Avlimil, herbal product without published clinical trials. Significant safety concern because primary component is sage leaf which can lead to neurotoxicity with prolonged use
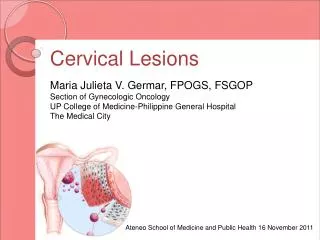
Identification of Common &Benign Cervical Lesions • Ectropion • Nabothian Cysts • Polyps (Endocervical vs prolapsing endometrial) • Obstetrical Lacerations • Cervical Warts (HPV you can see) • Infectious Causes: Cervicitis, Herpes, Chlamydia, Gonorrhea, Tricomoniasis, PID
Dralaamoshbah.blogspot.com • Ectropion
www.gynae.com sg • Polyp with long stalk
www.medscape.com • Obstetrical laceration or post-leep
Cervical Warts (HPV) • www.manbir-online.com
Deptswashington.edu • Cervicitis
www.nlm.nih.gov • Cervicitis
www.deptswash.edu • Chlamydial Cervicitis
Identification of Common Benign Cervical Lesions • Ectropion: normal at pubarche, w/ combination ocps, during pregnancy • Nabothian Cysts: Epithelial layer occluding gland opening • Endocervical polyp w/ thin clearly visible stalk may be removed. Endometrial should be referred. • Obstetrical lacerations exist & require no TX • Infectious causes should be treated