Download
1 / 33
330 likes | 590 Views
Emergency Contraception A Well Kept Secret. Tony Ogburn, MD University of New Mexico Health Sciences Center. Objectives. Understand the need for EC Review the current methods of EC available in the U.S. Understand the barriers to use that exist for EC.

E N D
Emergency Contraception A Well Kept Secret Tony Ogburn, MD University of New Mexico Health Sciences Center
Objectives • Understand the need for EC • Review the current methods of EC available in the U.S. • Understand the barriers to use that exist for EC. • Be familiar with approaches to improve EC utilization.
The few things I really want you to know! • What form of EC is most effective • Talk to every reproductive age woman at risk for pregnancy about EC • Provide EC in advance • Support EC to be available over the counter.
A 27 yo G3 P3, married patient calls your office saying she and her husband noted the condom was broken after sex the night before. What should she do??
The Setting • ~3.0 million unintended pregnancies annually • half (48%) of all pregnancies • Half (48%) of women aged 15-44 have had an unintended pregnancy • Unintended pregnancy is a major public health problem that affects individuals and society • Emergency contraception has the potential to reduce unintended pregnancy significantly Source: Henshaw 1998, Trussell et al. 1997
3 Million Unintended Pregnancies • ONE HALF . . .couples using no method of contraception 3 million couples • ONE HALF. . .couples using a reversible method imperfectly, or experiencing a method failure24 million couples Source: Henshaw 1998; Abma et al. 1997
EC: Potential Impact • Reduce unintendedpregnancies by 1.5 million • Reduce abortions 0.7 million Source: Trussell et al. 1992; Henshaw 1998
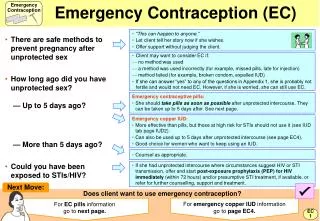
Emergency Options in theUnited States • Oral contraceptive pills containing only progestin • Oral contraceptive pills containing estrogen and progestin • Emergency Copper-T IUD insertion
Emergency Contraceptive Pills: Combined • Regular birth control pills- Yuzpe method • Contain estrogen and progestin- at least 1mg of LNG and 200mcg of ethinyl estradiol • 2 doses of 2, 4, or 5 pills, depending on brand • First dose within 72(120) hours • Second dose 12 hours later(or maybe not!) • Side effects: nausea (50%) and vomiting (20%) Trussell et al. Women’s Health Prim Care 1998;1:55
Emergency Contraceptive Pills: Combined Preven (No longer available)
Emergency Contraceptive Pills: Progestin-only • Birth control pills containing only progestin • 2 doses of 1 Plan B tablet or 20 Ovrette tablets • First dose within 72(120) hours after intercourse • Second dose 12 hours later(or maybe not!) • Less nausea/vomiting than combined ECPs Task Force. Lancet 1998;352:428
Emergency Copper IUD Insertion • Copper-T IUD (ParaGard) • Insertion within 5 days after unprotected intercourse • 10 more years of highly effective contraception • Much more effective than ECPs • Not recommended for women at risk of sexually transmitted infections (STIs)
Copper-T IUD Ortho
Combined ECP Effectiveness: Single Use 100 women have unprotected sex in the 2nd or 3rd week of their cycle 8 will become pregnant without emergency contraception 2 will become pregnant using combined ECPs (75% reduction) Source: Trussell, Rodríguez and Ellertson 1998
Progestin-only ECP Effectiveness: Single Use 100 women have unprotected sex in the 2nd or 3rd week of their cycle 8 will become pregnant without emergency contraception 1 will become pregnant using progestin ECPs (88% reduction) Source: WHO 1998
IUD Effectiveness - Single Use 1000 women have unprotected sex in the 2nd or 3rd week of their cycle 80 will become pregnant without emergency contraception 1 will become pregnant after IUD insertion (99% reduction) Source: Trussell and Ellertson 1995
Emergency Contraceptive Effectiveness If 1000 women have unprotected sex once in the second or third week of their cycle
Concerns about EC • It’s an abortion pill • It will keep woman from using more effective means of contraception and have “risky sex” • It’s not safe and can cause serious side effects
Definition of Pregnancy • NIH/FDA • Pregnancy encompasses the period of time from confirmation of implantation until expulsion or extraction of the fetus. • ACOG • Pregnancy is the state of a female after conception and until termination of the gestation. Conception is the implantation of the blastocyst. It is not synonymous with fertilization; it is synonymous with implantation. Source: US Government 1983; Hughes 1972
Mechanisms of Action • Inhibit ovulation • Trap sperm in thickened cervical mucus • Inhibit tubal transport of egg or sperm • Interfere with fertilization, early cell division, or transport of embryo • Prevent implantation by disrupting the uterine lining
Does Providing ECPs Increase Risk-Taking? • Three randomized trials comparing advance provision vs. education only • Use was appropriate • Patients did not abandon or decrease the use of their regular contraceptives • Decrease in unintended pregnancies
Safety • No evidence based contraindications to progestin only ECP or IUDs • Four case reports of cerebrovascular accidents with combined ECP
Other issues • How long after is too long? • One dose or two? • Nausea/vomiting • Spotting • Starting contraception • Menses
How Long After the Morning After? • Initial recommendations were to administer first dose within 72 hours • Several trials have found no decrease in efficacy if given within 120 hours von Hertzen et al, Lancet, 2002, Ellertson et al, Obstet Gynecol, 2003
One dose or two? • Recommendations call for two doses 12 hours apart • Studies indicate that giving the same total as one dose is as effective von Hertzen et al, Lancet, 2002, Ellertson et al, Obstet Gynecol, 2003
Reducing the Risk of Nausea • Meclizine significantly reduces the risk of nausea and vomiting associated with the Yuzpe regimen of emergency contraception. • Significantly increases the risk of drowsiness. Raymond et al. Obstet Gynecol 2000;95:271
Spotting Ellertson et al. Obstet Gynecol 6/2003
Number of Days of Spotting Ellertson et al. Obstet Gynecol 6/2003
Starting contraception after EC Oral contraceptives, patches, and vaginal rings • Regular start: use backup until next period, then begin pills/patches/rings according to regular patient instructions • Jump start: take 2 ECP doses. Start a new pack of OCs, or use a patch/ring the next day (use backup for first 7 days)
Starting contraception after EC Depo-Provera® • Regular start: use backup until next period, then start Depo-Provera according to regular patient instructions • Jump start: take 2 ECP doses. Start Depo-Provera the next day (use backup for first seven days)
Menses after ECP Use • Similar for combined and progestin-only regimens • Relative to anticipated onset of next menses • 13% have a delay of 8+ days • 15% have a delay of 4-7 days • 61% have menses within 3 days • 11% have early onset (>3 days early) • A follow-up visit is warranted if menses do not return within three weeks following treatment Source: WHO 1998